EMT Lecture - OB/GYN & Neonatal Care
Understanding Female Reproductive Anatomy
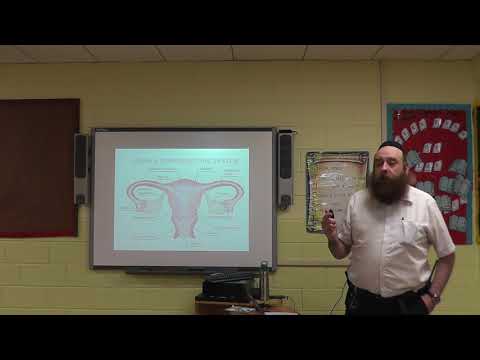
Overview of Key Structures
- The uterus, referred to as the womb, is centrally located in the female reproductive system.
- Ovaries are positioned on either side of the uterus and are connected by fallopian tubes.
- Pregnancy is intended to occur within the uterus; it serves as a closed system with minimal openings.
Uterine Functionality
- The cervix has a small opening known as the cervical os, allowing only fluids and sperm to pass through.
- The endometrium is the uterine lining that detaches monthly if fertilization does not occur, leading to menstruation.
Egg Development and Menstruation
Egg Lifecycle
- Females are born with a finite number of eggs in each ovary; no new eggs are produced after birth.
Monthly Cycle
- An egg travels from an ovary through a fallopian tube into the uterus; fertilization can lead to embryo formation or result in menstruation if unfertilized.
Anatomy of Female Orifices
Understanding Body Openings
- Three main orifices: bladder (urination), vagina (birth canal), and rectum (defecation).
- During childbirth, multiple bodily substances may be expelled simultaneously due to pressure from the baby.
Placenta Formation and Function
Role of Placenta
- The placenta develops during pregnancy, providing nutrients from mother to fetus while removing waste products.
Connection Details
- It connects via tiny blood vessels attached to the uterine wall, facilitating nutrient exchange between mother and child.
Stages of Labor
Initial Stage Insights
Understanding Labor Stages and Risks
The Role of Contractions in Labor
- Contractions during pregnancy serve to dilate the cervix, allowing for the passage of the baby. This process is crucial as it prepares the body for delivery.
- Cervical dilation is a key focus during labor; contractions are responsible for this dilation, which is essential for childbirth.
- Full cervical dilation is defined as ten centimeters, marking a significant milestone in the labor process.
Stages of Labor
- The first stage of labor begins with contractions and ends when the cervix is fully dilated (10 cm).
- The second stage starts with full cervical dilation and concludes with the birth of the child.
- The third stage begins after birth and ends with the delivery of the placenta, completing the birthing process.
High-Risk Factors in Pregnancy
- Antepartum risks include maternal age (under 16 or over 40), previous miscarriages, and post-term gestation (beyond 42 weeks).
- Drug use or medications during pregnancy can pose significant risks to both mother and child.
- Gestational diabetes may develop in non-diabetic women during pregnancy, typically tested around months five or six.
Understanding Amniotic Fluid
- Amniotic fluid surrounds the baby within the uterus, providing a protective environment.
- A mucus plug helps retain amniotic fluid within the uterus, preventing leakage while pregnant women walk.
Ectopic Pregnancy Awareness
- EMT protocols dictate that unexplained abdominal pain in females of childbearing age should raise suspicion for ectopic pregnancy.
- An ectopic pregnancy occurs when a fertilized egg implants outside its normal location, often in a fallopian tube.
Understanding Ectopic Pregnancy and Preeclampsia
Ectopic Pregnancy Overview
- Ectopic pregnancy poses a life-threatening risk for females of childbearing age, often going unnoticed until severe symptoms arise.
- Symptoms may include unexplained abdominal pain, typically on one side, which can occur as early as four to six weeks into the pregnancy.
- Medical professionals should suspect ectopic pregnancy in women aged 16 to 64 presenting with unilateral abdominal pain, especially if they are of childbearing age.
- Serious complications can arise from ectopic pregnancies, including internal bleeding and potential loss of an ovary if not diagnosed promptly.
- Early detection is crucial; failure to identify an ectopic pregnancy can lead to severe hemorrhaging and even death.
Recognizing Signs of Preeclampsia
- Pregnant women undergo frequent check-ups primarily to monitor blood pressure and test urine for protein levels, which are critical for identifying preeclampsia.
- High blood pressure readings (over 160/110 mmHg) indicate preeclampsia; immediate medical assistance is necessary in such cases.
- The term "toxemia" is synonymous with preeclampsia; it refers to the presence of high protein levels in urine during pregnancy.
- Common symptoms of preeclampsia include visual disturbances, nausea, vomiting, upper quadrant pain, headaches, and confusion.
Understanding Preeclampsia and Eclampsia
Key Differences Between Preeclampsia and Eclampsia
- Preeclampsia, if untreated, can progress to eclampsia. The critical distinction is that eclampsia includes seizures, while preeclampsia does not.
- In exams, the presence of seizures indicates eclampsia; absence of seizures suggests preeclampsia. This differentiation is crucial for diagnosis.
Case Study: Consequences of Ignoring Symptoms
- A notable incident involved EMTs neglecting a call about a pregnant woman in distress due to their lunch break, leading to severe consequences.
- The patient transitioned from preeclampsia to eclampsia and ultimately died, highlighting the importance of timely medical intervention.
Recognizing Signs of Preeclampsia
- Blood pressure readings above 160/110 mmHg are indicative of hypertension associated with preeclampsia. Visual disturbances may also be present.
- It’s essential to manage preeclampsia effectively to prevent it from escalating into eclampsia.
Braxton Hicks Contractions Explained
- Braxton Hicks contractions are false labor pains that can occur before actual contractions begin. They are not real contractions but can cause confusion.
- Pregnant women may not always recognize these as false contractions; thus, EMTs should be aware when transporting expectant mothers.
Hypotensive Syndrome in Pregnancy
- Hypotensive syndrome often occurs when pregnant women lie supine during transport, which compresses the inferior vena cava against the spine.
- Many pregnant women know they shouldn't lie on their backs; however, EMT practices sometimes overlook this important guideline.
Best Practices for Transporting Pregnant Women
- EMT protocols should prioritize positioning pregnant patients on their sides rather than supine during transport to avoid hypotension.
- An anecdote illustrates the negative impact of improper positioning during transport—EMTs must be trained to avoid such mistakes.
Understanding Obstetric Emergencies
Key Concepts in Obstetric Care
- Discussion on patient seating in an ambulance, emphasizing safety protocols and the importance of securing patients properly during transport.
- Introduction to abruptio placentae, a condition where the placenta detaches from the uterine wall, leading to bleeding. This is a critical emergency that requires immediate attention.
- Explanation of placenta previa, where the placenta covers the cervix, complicating delivery. The speaker highlights its implications for vaginal birth and potential need for cesarean section.
- Mention of varying medical opinions regarding cesarean sections and induction methods, indicating differing practices among healthcare providers.
Assessing Pregnancy Status
- Importance of asking women about their pregnancy status; however, caution is advised due to potential sensitivities surrounding this question.
- Clarification on how pregnancy duration is measured: weeks versus months. Emphasizes confusion often experienced by patients regarding their exact gestational age.
- Discussion on common questions to assess pregnancy progress, including contractions and any bleeding or discharge present.
Understanding Gravida Terms
- Definitions of obstetric terms: primigravida (first-time pregnant woman) vs. multigravida (woman who has been pregnant multiple times), which are essential for understanding patient history.
- Importance of knowing how many pregnancies resulted in live births as part of assessing maternal health and risks involved in current pregnancy.
Signs of Imminent Delivery
- Questions to determine if a woman is close to delivering include whether she feels the urge to push or has a strong need to use the bathroom—indicators that labor may be imminent.
- Inquiry into prenatal care received by the patient and knowledge about her last menstrual period (LMP), which helps estimate gestational age more accurately than self-reported months.
Recognizing Labor Progression
- Addressing concerns EMT personnel have about determining if delivery will occur at home or if there’s time to reach a hospital safely; emphasizes recognizing key signs of labor progression.
- Description of "umbilical bungee," an alarming situation where a baby is delivered while still attached via umbilical cord during transport—a scenario that must be avoided at all costs.
Trusting Maternal Instinct
- Acknowledgment that mothers often know when they are going into labor better than anyone else; their intuition should be trusted especially if they have previous experience with childbirth.
- Importance of listening carefully when mothers report that "the baby is coming," particularly for those who have had prior deliveries—they can provide crucial insights into their condition.
Monitoring Contractions
- Guidelines for timing contractions: measure both frequency and duration. If contractions are less than two minutes apart lasting 45 seconds or longer, it indicates imminent delivery.
Delivery Protocols and Considerations
Managing Labor and Delivery in Emergency Situations
- Pregnant women may instinctively grab onto nearby objects or people during contractions; it's crucial to monitor their condition closely.
- Avoid allowing pregnant women to use the bathroom alone, as complications can arise, such as delivering a baby in an unsuitable location.
- An OBGYN kit is essential for deliveries; it typically includes surgical tools like scalpels and scissors, which are vital for safe delivery procedures.
Ensuring Privacy and Safety During Delivery
- Maintaining the mother's privacy is important; there have been instances where deliveries occurred in public spaces, necessitating quick action from EMTs.
- In one case, a mother delivered her baby in an ambulance after being transported from a public area. The environment significantly impacted the outcome of the delivery.
Preparing for Delivery
- Positioning the mother comfortably is key; she can be semi-Fowler's or supine based on her comfort level during labor.
- Always carry two OBGYN kits to ensure you have backup supplies since materials may fail during critical moments.
Recognizing Imminent Deliveries
- Crowning indicates imminent delivery; if visible, immediate action is required without internal examinations unless absolutely necessary.
- Do not allow mothers to go to the bathroom or hold their legs together if delivery seems imminent—stay on site for assistance.
Understanding Normal Delivery Procedures
- A normal cephalic delivery occurs when the baby's head appears first. The first shoulder's emergence poses challenges that require careful handling.
- Suctioning the baby's mouth and nose immediately after birth is crucial for ensuring proper breathing and thermoregulation.
Post-delivery Care Essentials
- After birth, keeping the baby warm and dry is vital due to their immature skin's inability to regulate temperature effectively.
Delivery Complications and Management
Overview of Delivery Kit
- The delivery kit includes essential tools such as surgical scissors, a scalpel, suction devices, clamps, sanitary napkins, and wraps for the baby.
- Franklin successfully cut the umbilical cord without complications; all aspects of the delivery were healthy.
Handling Unruptured Amniotic Sac
- A common complication is an unruptured amniotic sac where the baby appears to have a "stocking" over its face.
- EMTs should avoid using metal instruments to break the sac; instead, they can use their fingers to rupture it gently.
- Breaking the sac will create a mess with amniotic fluid; therefore, it's crucial to manage this carefully during delivery.
Nuchal Cord Management
- Another potential issue is when the umbilical cord is wrapped around the baby's neck (nuchal cord). This does not affect breathing while in utero but becomes critical once delivered.
- If tight around the neck after birth, EMTs should lift it over the baby's head or cut it if necessary.
Post-delivery Care
- After delivery, keeping the baby warm is vital. Normal bleeding post-delivery can be about 500 ml (half a liter).
- To help stop bleeding: allow mother and baby to bond quickly and massage the uterus gently.
Uterine Massage Techniques
- In hospital settings, uterine massage may occur internally by trained professionals; however, this practice isn't suitable in field conditions.
Understanding Apgar Score
Neonatal Resuscitation Techniques
Importance of Understanding Neonatal Care
- The speaker emphasizes the significance of knowledge from the neonatal resuscitation program, highlighting that EMTs often lack this critical information.
- Upon birth, immediate actions include cleaning, stimulating, and ensuring sterility while suctioning the mouth if necessary.
Assessing Vital Signs
- After initial care, maintaining warmth is crucial; finding a vital sign quickly is essential for determining treatment plans.
- To assess heart rate in a newborn, place a stethoscope over the baby's heart to detect rapid beats effectively.
Heart Rate Assessment Methodology
- A six-second count of heartbeats can be multiplied by ten to determine the heart rate (e.g., 6 beats = 60 bpm).
- Normal heart rates are categorized:
- Greater than 100 bpm indicates a healthy baby.
Treatment Based on Heart Rate
- For babies with a heart rate above 100 bpm, provide "blow-by" oxygen without direct contact to avoid eye exposure.
- If the heart rate is below 100 bpm but above 60 bpm, use a neonate bag-valve-mask (BVM) at 15 liters every three seconds.
Emergency Procedures for Critical Conditions
- A heart rate below 60 bpm necessitates neonatal CPR using a specific technique: three compressions followed by one breath (3:1 ratio).
- The speaker stresses understanding these procedures as they form part of essential neonatal care protocols.
Neonatal Resuscitation Triangle Concept
- The triangle illustrates that all newborns require warmth, drying, positioning, suctioning, and stimulation as foundational care steps.
- Advanced interventions like oxygen therapy or chest compressions are rare and typically not required for most cases.
Challenges in Abnormal Deliveries
- Breech deliveries present significant challenges; it’s advised to transport mothers quickly to hospitals for professional assistance.
Emergency Situations in Childbirth
Managing Nuchal Cord Complications
- Urgent intervention is required when the umbilical cord is compressed, as it can jeopardize the baby's oxygen supply. The baby relies on the cord until its first breath.
- In cases of nuchal cord (cord around the neck), manual repositioning of the baby's head may be necessary to relieve pressure on the cord. This requires careful insertion into the birth canal.
- Maintaining this position may be critical until reaching an emergency room or operating room, where surgical assistance can take over.
Addressing Excessive Bleeding
- Excessive bleeding during childbirth (over 500cc) necessitates immediate action, such as uterine massage to slow down blood loss and treating for shock if needed.
- The term "abortion" encompasses both medical procedures and spontaneous miscarriages; however, terminology sensitivity is important in patient care.
Handling Multiple Births
- Understanding twin deliveries involves recognizing that identical twins share one placenta while fraternal twins have separate placentas. This distinction is crucial for monitoring maternal and fetal health.
Care for Premature Infants
- Anticipate respiratory depression in infants born to addicted mothers; readiness to provide resuscitation measures is essential.
- Preterm infants require heightened care: protection from infection, warmth maintenance, and clear airways are vital for their survival.
Recognizing Meconium Aspiration Risks
- Stress during pregnancy can lead to meconium-stained amniotic fluid, which poses risks if aspirated by the baby during delivery.
- It’s important to inquire about the color of amniotic fluid upon rupture; green or yellow indicates potential meconium presence that could complicate neonatal outcomes.