Fisiología Renal - Concentración y Dilución orina(Multiplicador contracorriente)(IG:@doctor.paiva)
Concentration and Dilution of Urine in Renal Physiology
Introduction to Renal Physiology
- The class focuses on urine concentration and dilution, emphasizing the countercurrent system.
- Key topics include osmotic gradients, urea recycling, and countercurrent exchange mechanisms.
Understanding Osmolarity
- Two types of nephrons are identified: cortical and juxtamedullary, crucial for urine concentration.
- The flow direction of tubular fluid is opposite to that of blood in capillaries, essential for understanding renal function.
- Plasma osmolarity is approximately 300 mOsm/L; sodium chloride primarily contributes to this value.
Mechanisms of Urine Concentration
- A distinction is made between hyperosmolar (concentrated) and hypoosmolar (diluted) urine based on osmolarity changes relative to plasma.
- When a liquid loses osmolarity, it dilutes; when it gains osmolarity, it concentrates—fundamental concepts for renal physiology.
Body Responses to Water Balance
- In dehydration, plasma solute concentration increases, triggering ADH release from the hypothalamus to conserve water.
- Conversely, excess water decreases plasma solute concentration leading to reduced ADH secretion and increased urine volume.
Urine Production Variability
- Kidneys can produce highly concentrated urine (up to 1400 mOsm/L with low volume) or very dilute urine (down to 50 mOsm/L with high volume).
- The regulation of urinary osmolarity is primarily controlled by ADH levels in response to hydration status.
Summary of Hormonal Effects on Urination
- Increased ADH leads to more water reabsorption resulting in concentrated urine; decreased ADH results in diluted urine.
- Changes in solute excretion do not directly correlate with changes in solute concentrations but rather reflect water balance adjustments.
Gradients in Renal Osmolarity
- The lecture introduces the cortico-medullary osmotic gradient as vital for kidney function regarding fluid balance.
Osmolarity in Renal Cortex and Medulla
Osmolarity Gradients
- The osmolarity of the renal interstitium increases progressively from the cortex to the medulla, reaching levels between 600 to 1200 mOsm/L depending on whether the nephron produces concentrated or diluted urine.
Mechanisms of Hyperosmolar Interstitium
- The renal medullary interstitium is hyperosmolar due to mechanisms such as countercurrent multiplication and recycling of solutes, which help maintain osmotic gradients without directly increasing medullary osmolarity.
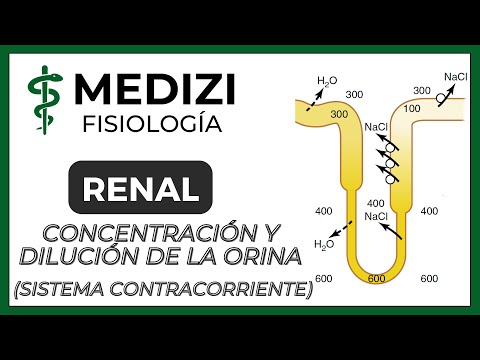
Countercurrent Multiplication Explained
- Countercurrent multiplication is a mechanism that transfers substances between two fluids flowing in opposite directions, crucial for creating osmotic gradients in the kidney.
Steps of Countercurrent Multiplication
- Unique Effect:
- Sodium chloride (NaCl) moves into the interstitium from the ascending limb while water moves out from the descending limb, concentrating tubular fluid.
- Fluid Flow Dynamics:
- As new fluid enters through filtration, it pushes existing fluid along, maintaining continuous flow and concentration changes throughout different segments of the nephron.
- Water Movement:
- Water drawn into the interstitium does not dilute it because it is quickly absorbed by vasa recta (straight vessels), preserving hyperosmolar conditions.
- Repetition of Processes:
- This cycle repeats continuously with each pass through the loop of Henle, gradually trapping more solutes in the medulla than water due to rapid absorption by vasa recta.
- Hormonal Influence:
Understanding Urea Recycling and Osmolarity in the Renal Medulla
Mechanisms of Urea Concentration and Reabsorption
- The process of countercurrent multiplication enhances concentration gradients, significantly increasing interstitial osmolarity due to antidiuretic hormone (ADH) effects, reaching levels between 1200 to 1400 mOsm/L.
- Urea contributes 40-50% to interstitial osmolarity; it is passively reabsorbed into the interstitium via specific transporters in the renal tubules.
- Plasma urea concentration influences its urinary excretion; higher plasma levels lead to increased urea expression, which is also affected by glomerular filtration rates.
- In renal insufficiency, decreased glomerular filtration results in elevated plasma urea concentrations, facilitating its excretion despite reduced kidney function.
- Tubular reabsorption of urea is influenced by ADH; higher ADH levels increase urea reabsorption while lower levels decrease it, affecting overall osmolarity.
Role of Collecting Duct and Countercurrent Exchange
- In the medullary collecting duct, water is reabsorbed under ADH influence while urea remains concentrated due to impermeability in certain segments.
- As fluid moves through the collecting duct under ADH influence, water is absorbed but not urea, leading to increased urea concentration within the tubular fluid.
- Urea undergoes a recycling process where it is both reabsorbed into the interstitium and secreted back into the tubules, contributing to osmotic gradients essential for urine concentration.
Importance of Vasa Recta in Maintaining Osmolarity
- The vasa recta play a crucial role in maintaining medullary hyperosmolarity by preventing rapid washout of solutes from the renal medulla through their low blood flow rate (5% of total renal blood flow).
- In presence of high ADH levels, maximum reabsorption occurs with osmotic gradients reaching up to 1200 mOsm/L; without ADH, most urea gets excreted leading to lower osmolarity around 600 mOsm/L.
- Sodium chloride (NaCl) generates half of medullary osmolarity while urea accounts for another half; this balance is critical for effective urine concentration mechanisms.
Mechanisms of Countercurrent Multiplication and Urine Concentration
Overview of Countercurrent Multiplication
- The process of countercurrent multiplication increases interstitial osmolarity with the help of urea and hydrogen ions, facilitating rapid water reabsorption into systemic circulation through straight vessels.
- Antidiuretic hormone (ADH) plays a crucial role by enhancing water permeability in the distal tubule and collecting duct, as well as increasing urea permeability in the medullary collecting duct.
Role of Sodium and Potassium Transport
- The transport mechanisms involve sodium-potassium chloride co-transporters in the thick ascending limb, which significantly enhance water reabsorption alongside urea.
- ADH release leads to concentrated urine formation; water is reabsorbed primarily at the end of the distal tubule and throughout both cortical and medullary collecting ducts.
Formation of Concentrated Urine
- In conditions where ADH is present, significant amounts of both water and urea are reabsorbed in the medullary collecting duct, leading to high osmolarity levels (1200 to 1400 mOsm/L).
Mechanism Behind Dilute Urine Production
- When ADH is absent, countercurrent multiplication still occurs but without water reabsorption; this results in dilution within tubular fluid due to sodium chloride absorption only.
- The osmolarity can drop significantly (as low as 50 mOsm/L), despite high volumes of urine being produced due to excess water relative to solutes like urea.
Summary Comparisons: With vs. Without ADH
- A comparison shows that urine with ADH has lower volume, higher osmolarity, and less pure water content compared to urine without ADH which has greater volume but lower osmolarity due to excessive dilution from large amounts of pure water.