dispe
Introduction to Functional Disorders of the Digestive System
Overview of Presentation
- The speaker, Dr. Parra, introduces the topic of functional disorders in the digestive system, specifically focusing on dyspepsia and irritable bowel syndrome (IBS) as common conditions.
Understanding Dyspepsia
- Dyspepsia is characterized by recurrent episodes of abdominal pain or discomfort localized in the upper digestive tract, particularly in the epigastric area. It accounts for 30% of gastroenterology consultations. Symptoms include flatulence, early satiety, nausea, belching, and heartburn.
Types of Dyspepsia
- Uninvestigated Dyspepsia: This refers to cases where no laboratory tests are conducted to identify the cause; for example, a young patient with four weeks of symptoms may be treated with proton pump inhibitors without further testing.
- Investigated Dyspepsia: Involves conducting tests like endoscopy to find an underlying cause such as peptic ulcers or gastric cancer. If all tests return normal results, it is classified as functional dyspepsia (70% of cases).
Criteria for Diagnosing Functional Dyspepsia
- Diagnosis relies on Rome IV criteria which require at least one symptom from a list including postprandial fullness and epigastric pain while ensuring no structural disease is present (normal endoscopy).
Role of Helicobacter Pylori
- A breath test can be used to check for Helicobacter pylori infection in patients with symptoms lasting eight weeks without alarm signs; treatment follows if positive results are found. If symptoms persist after eradication therapy, it indicates functional dyspepsia rather than organic causes.
Subtypes of Functional Dyspepsia
Distress Postprandial Syndrome vs Epigastric Pain Syndrome
- Two subtypes exist within functional dyspepsia:
- Postprandial Distress Syndrome: Characterized by symptoms like early satiety occurring three days a week over three months.
- Epigastric Pain Syndrome: Defined by symptoms such as burning or pain in the epigastrium.
Practical Differentiation Between Subtypes
- Patients with postprandial distress report feeling well when fasting but experience bloating after meals; this contrasts with those who have persistent epigastric pain regardless of meal timing.
Understanding Functional Dyspepsia and Its Symptoms
Differentiating Symptoms of Dyspepsia
- The distinction between postprandial distress syndrome and epigastric pain syndrome is highlighted, with the latter being characterized by relief after eating.
- Postprandial distress is triggered by food intake, while symptoms in epigastric pain syndrome improve following meals.
Pathophysiology of Functional Dyspepsia
- The complex pathophysiology involves multiple factors, including a brain-gut axis where mental stress affects intestinal function.
- Gastrointestinal motility disorders are prevalent, affecting up to 60% of patients; gastric accommodation issues can lead to symptoms due to inadequate relaxation of the stomach's fundus.
Gastric Accommodation and Sensitivity
- In functional dyspepsia patients, food may not be properly accommodated in the stomach, leading to congestion similar to traffic jams.
- Visceral hypersensitivity is discussed as a condition where patients have an abnormally low threshold for perceiving discomfort from minor stimuli.
Impact of Psychological Factors
- Psychological factors such as stress, anxiety, and depression play significant roles in functional dyspepsia cases.
- A thorough clinical history is essential for ruling out organic causes; laboratory tests may include blood counts and liver profiles.
Diagnostic Approach for Dyspepsia
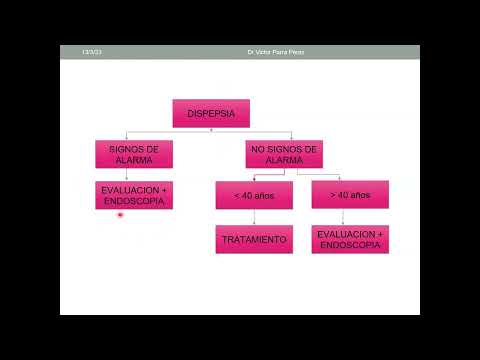
- Initial evaluation should focus on alarm signs (e.g., anemia or vomiting), which necessitate endoscopy.
- For patients under 40 without alarm signs, a therapeutic trial with proton pump inhibitors may be appropriate; those over 40 typically require endoscopy due to increased cancer risk.
Treatment Strategies for Functional Dyspepsia
- Treatment options include empirical antisecretory therapy with proton pump inhibitors showing efficacy in 40%-70% of cases.
- Prokinetics like metoclopramide or mosapride can be used specifically for postprandial distress syndrome management.
Non-Invasive Testing Options
- Non-invasive tests for Helicobacter pylori infection include fecal antigen tests and breath tests; breath testing is preferred due to its ease of use.
Treatment Approaches for Functional Dyspepsia
First-Line and Second-Line Treatments
- Prokinetics improve gastric emptying and accommodation; however, proton pump inhibitors (PPIs) are recommended for epigastric pain syndrome. If PPIs fail to relieve symptoms, tricyclic antidepressants become the second-line treatment.
- Amitriptyline is highlighted as a primary option among tricyclic antidepressants for treating postprandial syndrome when prokinetics do not alleviate symptoms.
Diagnostic Algorithm for Dyspepsia
- The diagnostic approach begins with evaluating alarm signs or high cancer risk indicators. An abnormal endoscopy leads to targeted treatment based on findings like ulcers or gastritis.
- In cases without alarm signs, functional dyspepsia may be treated with a Helicobacter pylori test; if positive, eradication therapy is initiated. If negative, an 8-week course of PPIs is prescribed.
Treatment Efficacy and Considerations
- Many patients with functional dyspepsia do not respond to esomeprazole; combining it with prokinetics like limosapride can be beneficial before considering tricyclic antidepressants.
- Functional dyspepsia has a complex pathophysiology characterized by visceral hypersensitivity, necessitating diverse therapeutic algorithms tailored to underlying mechanisms.
Understanding Irritable Bowel Syndrome (IBS)
Prevalence and Risk Factors
- IBS predominantly affects women (2:1 ratio), with risk factors including depression, young age, history of bacterial gastroenteritis (e.g., Campylobacter infection), and recent antibiotic use disrupting gut microbiota.
Symptoms and Diagnosis Criteria
- IBS is defined by recurrent abdominal pain coupled with altered bowel habits—diarrhea, constipation, or alternating patterns—without any identifiable organic cause.
- Abdominal pain must occur at least once weekly over three months alongside two of the following: pain related to defecation, changes in stool frequency or form.
Pathophysiology Insights
- The condition's complexity includes motility disorders, visceral hypersensitivity similar to functional dyspepsia, psychological factors, local inflammatory phenomena at the microscopic level, intestinal flora disturbances, and food intolerances/allergies.
Clinical Evaluation
- A thorough clinical history and physical examination are essential for diagnosing IBS while ruling out organic causes.
Types of Bowel Habits in IBS
- Constipation involves hard stools and feelings of incomplete evacuation; diarrhea features increased frequency often accompanied by urgency. Normal bowel movements typically fall between types 3 to 5 on the Bristol stool scale.
Understanding Irritable Bowel Syndrome (IBS) and Colonoscopy Guidelines
Importance of Symptom Assessment in IBS
- The utility of a visual scale for patients helps differentiate between diarrhea and constipation, which influences treatment decisions for those with irritable bowel syndrome (IBS).
Indications for Colonoscopy in Suspected IBS
- Not all patients require a colonoscopy; specific indications include iron deficiency anemia, age over 45, or family history of colon cancer.
- Alarm signs such as weight loss, bleeding, chronic diarrhea, or lack of response to standard treatments necessitate a colonoscopy.
Age Considerations for Screening
- Patients over 45 years old are at increased risk for colon cancer; thus, screening is recommended at this age.
- For individuals with a family history of colon cancer, screening should begin 10 years prior to the age at which their relative was diagnosed.
Multifactorial Treatment Approach
- Treatment involves identifying dietary factors and managing emotional aspects like anxiety and depression while promoting healthy lifestyle changes.
Patient Education and Expectations
- It’s crucial to explain that IBS is a functional disorder that does not increase cancer risk but requires ongoing management rather than a cure.
Lifestyle Modifications
- Recommendations include proper sleep hygiene, healthy diet choices, avoiding alcohol and tobacco, and regular physical activity to improve intestinal function.
Symptom-Specific Management Strategies
- Treatment varies based on predominant symptoms: antidiarrheals like loperamide for diarrhea-predominant IBS; rifaximin can help reduce gas.
Pain Management Options
- For severe pain in IBS patients, selective antispasmodics may be prescribed alongside dietary adjustments like low FODMAP diets.
Second-Line Therapies
- If initial treatments fail to alleviate pain, tricyclic antidepressants such as amitriptyline may be considered as second-line options.
Managing Mixed Symptoms
- In mixed symptom cases (diarrhea/constipation), careful monitoring is essential when using laxatives or adjusting dietary plans based on current symptoms.
Psychological Support in Treatment
- Psychological therapies can aid in managing IBS symptoms by teaching relaxation techniques; probiotics may also provide relief from significant abdominal pain.
Understanding Abdominal Pain Location
- Patients often experience pain on either side of the abdomen due to the structure of the colon; education about this variability is important for reassurance.
Follow-Up Care Protocol
- Regular follow-up appointments are necessary to reassess symptom management strategies every few weeks to ensure effective treatment outcomes.
Understanding the Management of Irritable Bowel Syndrome
Importance of Patient-Doctor Relationship
- A strong patient-doctor relationship is crucial for effective treatment; patients must feel comfortable sharing adverse effects of medications.
- Trust in the physician enhances the likelihood of patient improvement, regardless of the physician's skills or medication quality.
Key Conclusions on Managing Irritable Bowel Syndrome
- Successful management begins with a confirmed diagnosis and clear communication about the functional nature of the disorder, emphasizing that it is manageable but not curable.
- Detailed medical history is essential to identify dietary and lifestyle changes that could alleviate symptoms, such as reducing intake of carbonated drinks and high-fat foods.
Dietary Adjustments and Lifestyle Changes
- Patients may need to eliminate lactose if they are intolerant, suggesting alternatives like lactose-free milk or soy milk. Discussing sleep habits is also important since poor sleep can trigger IBS symptoms.
- If symptoms persist despite lifestyle changes, pharmacological and psychological treatments may be necessary, including referrals to psychologists or psychiatrists for underlying issues like depression or anxiety.
Medication Management Based on Symptoms
- The choice of medication should align with predominant symptoms: antispasmodics for abdominal pain and laxatives for constipation are common options. Always inquire about patient expectations regarding symptom relief.
- Adjustments in medication dosages or types may be required based on ongoing discussions with patients about their comfort levels with current treatments.
Understanding Bristol Stool Scale in IBS Management
- The Bristol stool scale helps categorize bowel movements; understanding this can guide treatment decisions based on whether diarrhea or constipation predominates in a patient's condition.
- Flexibility in treatment approaches is necessary as IBS can present differently over time; alternating between diarrhea and constipation requires tailored interventions accordingly.
Monitoring Symptoms Over Time
- Regular assessments using tools like the Bristol scale allow physicians to track changes in bowel habits and adjust management strategies effectively based on current presentations (e.g., diarrhea vs constipation).
- Recognizing that IBS episodes vary significantly over time emphasizes the need for continuous monitoring and adaptation of treatment plans according to individual patient experiences.