PLEXO BRAQUIAL - PARTE 2
Understanding Muscle Abduction and Neuroanatomy
Clinical Presentation of Muscle Atrophy
- The subject presents with an inability to perform shoulder abduction, indicating a potential issue in the muscular or neurological function.
- Notable muscle atrophy is observed, suggesting underlying nerve involvement affecting movement.
Nerve Involvement in Abduction
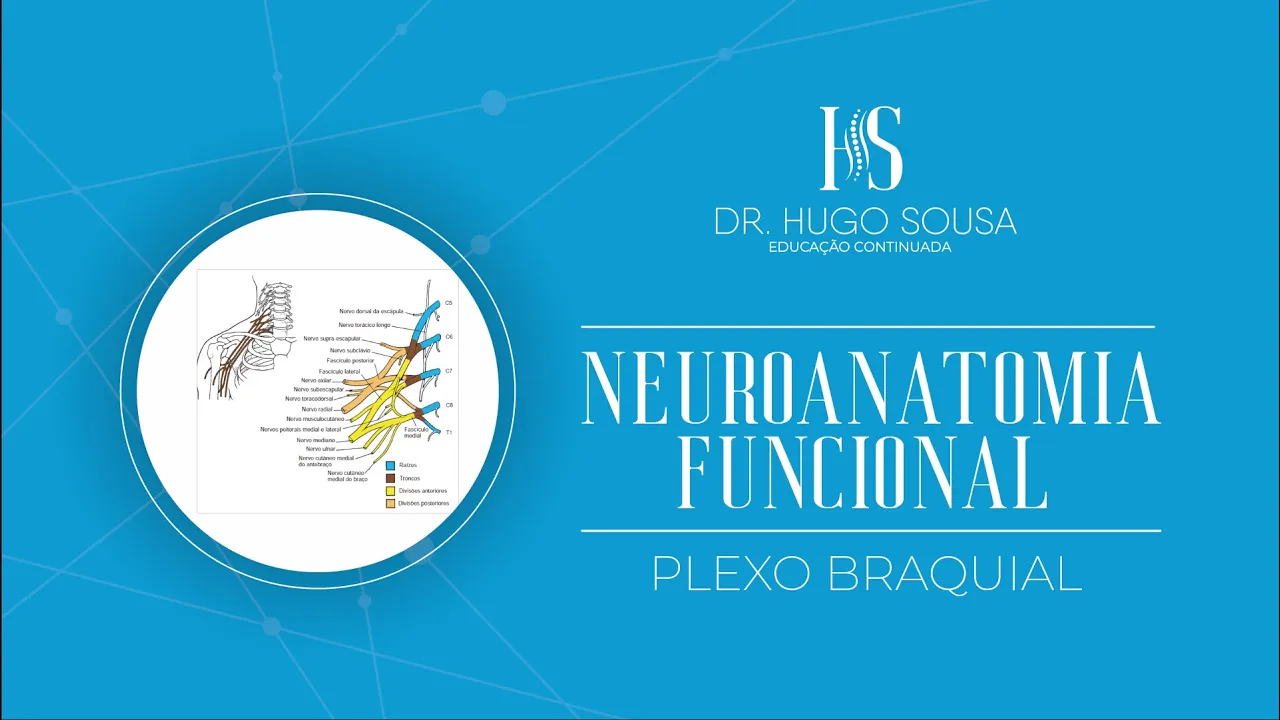
- Key nerves responsible for shoulder abduction include the axillary and suprascapular nerves, originating from spinal segments C5 and C6.
- Understanding these nerves is crucial for diagnosing conditions related to muscle weakness or sensory loss.
Importance of Electrophysiological Studies
- Electrophysiologists utilize functional exams like electromyography (EMG) to assess neuromuscular disorders.
- Patients may report symptoms such as paresthesias (tingling), weakness (paresis), fatigue, and diminished reflexes, which guide diagnostic processes.
Diagnostic Techniques: MRI vs. Electromyography
- While MRI provides anatomical insights, it does not assess functional aspects; EMG evaluates muscle activity during contraction.
- EMG helps measure electrical signals in muscles and nerves, essential for understanding neuromuscular health.
Dermatomes and Myotomes Overview
- Dermatomes are skin areas innervated by specific spinal nerve roots; understanding them aids in clinical assessments of sensory function.
- The upper limb's dermatomes correspond to spinal segments C3 through T1, critical for evaluating sensory deficits during examinations.
Assessing Sensory Function Through Dermatomes
Practical Examination Techniques
- During clinical tests, practitioners assess dermatomes to evaluate sensory integrity across the upper limb.
- Specific regions correlate with spinal segments; e.g., lateral arm corresponds to C5 while thumb sensation relates to C6.
Mapping Sensory Regions
- The examination includes identifying territories associated with various nerves like the axillary nerve around the shoulder area.
- Each finger has designated dermatomal levels that help pinpoint neurological issues based on sensation loss patterns.
Myotomes: Muscle Innervation Insights
Understanding Myotomes
- Myotomes refer to muscle groups innervated by specific spinal segments; they are vital for assessing motor function alongside dermatomes.
- Testing myotomes involves evaluating strength through movements like shoulder flexion or elbow extension linked to corresponding spinal levels.
Complexities of Joint Innervation
- Joints receive diffuse innervation from multiple nerves, complicating pain assessment due to overlapping sensory fields.
Testing Muscle Function and Reflexes
Assessing Elbow Joint Flexion
- The speaker discusses testing the flexion of the elbow joint, focusing on the biceps brachii muscle. The myotome responsible for this action is predominantly segment C6.
Testing Elbow Extension
- When testing elbow extension, the triceps brachii muscle is evaluated, with segment C7 being involved. This indicates a connection between specific movements and spinal segments.
Hand Movement Assessment
- The speaker explains how to assess hand movements such as abduction and adduction of fingers to test interosseous muscles (palmar and dorsal), which are linked to segment C8-T1.
Myotatic Reflex Testing
- Myotatic reflexes can be tested by tapping tendons with a hammer, leading to a reflexive contraction. This involves sensory innervation from muscle spindles and Golgi tendon organs.
Integrity Testing of Specific Muscles
- The integrity of muscles like the biceps can be tested by percussing their tendons. Similar tests can be performed on the triceps tendon, indicating functional assessments for these muscles.
Nerve Innervation and Muscle Functions
Axillary Nerve Territory
- Discussion includes the axillary nerve's territory affecting the deltoid region, emphasizing its role in shoulder movement and sensation in that area.
Median Nerve Innervation
- The median nerve's territory includes areas related to thumb movement (thenar region) and finger sensations, particularly involving segments C8-T1.
Overview of Spinal Segments and Nerves
- A detailed overview is provided regarding spinal segments associated with various nerves, including their motor functions and sensory roles across different muscle groups.
Specific Nerves and Their Functions
Dorsal Scapular Nerve
- Originating from segment C5, it innervates rhomboid major/minor muscles responsible for scapular adduction.
Long Thoracic Nerve
- This nerve arises from segments C5-C7; it innervates serratus anterior muscle crucial for scapular stabilization during arm movements.
Muscle Groups Involved in Shoulder Movement
Suprascapular Nerve
- Originating from upper trunk (C5-C6), it innervates supraspinatus (abducting shoulder) and infraspinatus (external rotation), both part of rotator cuff functionality.
Subclavian Nerve
- Also originating from upper trunk (C5-C6), this nerve innervates subclavius muscle which stabilizes clavicle position during shoulder activities.
Brachial Plexus Contributions
Lateral Pectoral Nerve
- Arising from lateral fascicle (C5-C7), it primarily innervates pectoralis major aiding in shoulder flexion/adduction while also contributing sensory information through cutaneous branches.
Nerve Innervation and Functions
Medial Cutaneous Nerve of the Arm
- The medial cutaneous nerve of the arm originates from the medial fascicle with spinal segments C8 and T1, providing sensory innervation to the skin on the medial side of the distal arm.
Medial Cutaneous Nerve of the Forearm
- This nerve also arises from the medial fascicle, serving spinal segments C8 and T1, and is responsible for sensory innervation to the skin on the medial side of the forearm.
Median Nerve Overview
- The median nerve originates from both medial and lateral fascicles with spinal segments C5, C6, and T1. It has motor functions for all muscles in the anterior compartment of the forearm except for specific exceptions.
Muscles Innervated by Median Nerve
- The median nerve innervates flexor carpi radialis, palmaris longus, flexor digitorum superficialis, pronator teres, and pronator quadratus. Notably, it does not innervate flexor carpi ulnaris or part of flexor digitorum profundus.
Thenar Region Innervation
- In addition to forearm muscles, it innervates thenar muscles including abductor pollicis brevis, flexor pollicis brevis (superficial head), and opponens pollicis.
Lumbrical Muscles Innervation
- The median nerve also supplies motor function to lateral two lumbricals (first and second), which originate from tendons of flexor digitorum profundus.
Sensory Function of Median Nerve
- Sensory functions include providing sensation to palm surface areas including half of fourth digit laterally. A simple way to remember its territory is through its relation to palmar surfaces.
Ulnar Nerve Functions
Ulnar Nerve Overview
- Originating from a medial fascicle with spinal segments C7, C8, and T1; it serves both motor and sensory functions.
Motor Functions
- It innervates intrinsic hand muscles excluding three thenar muscles; thus playing a crucial role in hand dexterity.
Intrinsic Hand Muscle Innervation
- All intrinsic hand muscles are supplied by ulnar nerve except for three thenar muscles (innervated by median). Additionally includes two lateral lumbricals.
Sensory Function of Ulnar Nerve
- Provides sensory input to palmar surface areas including fifth digit's palm region as well as dorsal aspects related to this area.
Subscapular Nerves Overview
Subscapular Nerves Description
- There are superior and inferior subscapular nerves originating from posterior fascicles with spinal segments C5-C6. Their primary function is motor control over specific shoulder muscles.
Specific Muscle Innervation
Overview of Shoulder Joint Muscles and Nerves
Key Muscles Involved in Shoulder Movement
- The subscapularis muscle is a significant adductor of the shoulder joint, emphasizing its importance in shoulder mechanics.
- The lower part of the subscapularis muscle is innervated by the inferior subscapular nerve, which originates from spinal segments C5-C6 and plays a crucial motor role.
- The axillary nerve, also originating from the posterior cord with spinal segments C5-C6, has both motor functions for muscles like the deltoid and sensory functions for skin over the upper lateral arm.
Functions of Major Shoulder Muscles
- The deltoid muscle facilitates various shoulder movements including flexion, abduction, extension, and external rotation.
- The rotator cuff comprises four key muscles: subscapularis, teres minor, infraspinatus, and supraspinatus; these are essential for stabilizing the shoulder joint.
Sensory Functions and Clinical Relevance
- The axillary nerve provides sensory innervation to the skin on the upper lateral aspect of the arm; this area is often used for intramuscular injections.
- The radial nerve is one of the largest nerves from the brachial plexus (C5-C6), responsible for motor function in all posterior compartment muscles of the arm and forearm.
Implications of Nerve Injuries
- Injury to the radial nerve can lead to significant functional impairments such as wrist drop or "wrist drop" syndrome due to loss of extensor function.