Sleep Physiology, Animation
Sleep and Its Stages
This section provides an overview of sleep as a temporary state of unconsciousness and introduces the different stages of sleep.
Sleep as a Natural Process
- Sleep is a temporary state of unconsciousness where the brain is primarily responsive to internal stimuli. It is different from other states of unconsciousness like coma or general anesthesia.
- Unlike those states, sleep is a natural, cyclic process that is self-regulated and easily reversible to wakefulness.
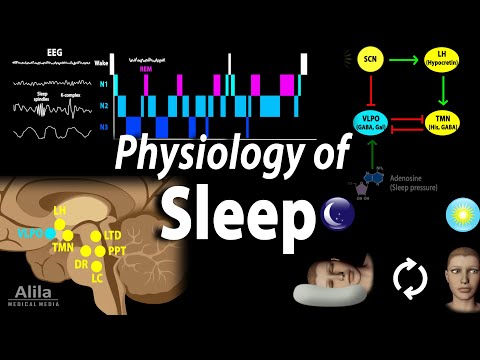
- Brain activity during sleep can be recorded using electroencephalogram (EEG), which measures electrical activities in the cerebral cortex.
Stages of Sleep
- Different stages of consciousness correspond to different types of brain waves.
- A fully awake and alert brain produces high-frequency low-voltage beta-waves. As consciousness decreases, brain waves become slower in frequency and higher in voltage.
- There are two major phases of sleep: rapid eye movement (REM) sleep and non-rapid eye movement (non-REM) sleep.
- Non-REM sleep progresses through three stages: N1, N2, and N3.
Stage N1
- N1 is the transitional state between wakefulness and sleep. The EEG is dominated by alpha-waves.
- The sleeper can be easily awakened with light stimulation. N1 typically lasts a few minutes.
Stage N2
- N2 is a deeper sleep state where stronger stimuli are required to produce awakening.
- Brain activity is slower and more irregular, with short bursts of "sleep spindles" and "K-complexes".
- Memory consolidation may occur during this stage.
Stage N3
- N3 is deeper than N2. Slow delta-waves dominate during this stage.
- Muscles relax, vital signs are at their lowest, and it is difficult to wake the sleeper.
- N3 is typically followed by a transition to N2 before REM sleep occurs.
Rapid Eye Movement (REM) Sleep
- REM sleep is characterized by rapid eye movements under the eyelids.
- Brain activity during REM sleep is similar to that of the waking state, hence it's called "paradoxical" sleep.
- Most dreams occur during REM sleep, and some autonomic reflexes are active.
- Skeletal muscles are inhibited during REM sleep to prevent acting out dreams.
Sleep Cycle
- The sequence of stages (N1, N2, N3, and REM) repeats itself 4 to 5 times in a typical night.
- As the night progresses, the duration of N2 and REM sleep increases while N3 decreases.
Regulation of Sleep
- The amount and timing of sleep are regulated by two major factors: homeostatic drive and circadian rhythm.
- Homeostatic drive refers to the body's need for sleep or pressure to sleep. It builds up as we awaken and decreases after a good night's sleep.
- Adenosine is thought to be a substance that accumulates with waking hours and drives the pressure to sleep. Caffeine acts as an antagonist of adenosine, promoting wakefulness.
- Circadian rhythm is the body's biological clock for the sleep-wake cycle. It determines the timing of sleep.
- The suprachiasmatic nucleus (SCN) in the hypothalamus serves as the master clock for circadian rhythm. Light inputs from the retina reset this clock daily according to the day-night cycle.
Sleep-Wake Switch Mechanism
- The ventrolateral preoptic nucleus (VLPO) in the hypothalamus plays a role in promoting sleep.
- The SCN inhibits the VLPO during the day, while adenosine activates it.
- GABA is used by the VLPO to inhibit wake-promoting regions of the brain, including nuclei in the reticular formation and posterior hypothalamus.
- The tuberomammillary nucleus (TMN) and hypocretin neurons are important for maintaining wakefulness. Mutual inhibition between TMN and VLPO forms the basis of the sleep-wake switch mechanism.
- Loss of hypocretin neurons can result in narcolepsy.
Sleep-Wake Cycle
- During the day, the SCN inhibits VLPO and stimulates hypocretin neurons, promoting wakefulness.
- By the end of the day, when SCN activity is lowest and pressure to sleep is highest, VLPO is activated, initiating sleep.