EMT Lecture - Pathophysiology of Ventilation, O2, & Airway Management
Pathophysiology of Ventilation and Respiratory Emergencies
Overview of Breathing Mechanism
- The discussion focuses on the mechanics of breathing, including how and why we breathe, along with associated pathophysiological conditions.
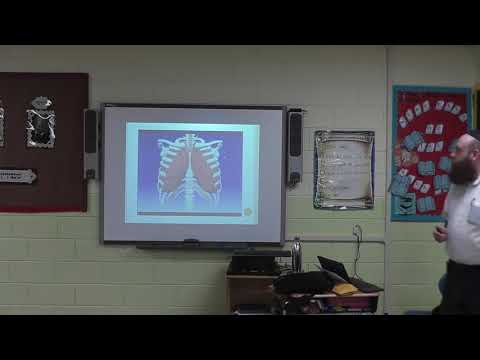
Anatomy of the Respiratory System
- Air enters through the nose and mouth; the nasal pharynx is located behind the nose, while the oral pharynx is behind the mouth.
- The epiglottis prevents foreign bodies from entering the trachea; below it lies the larynx, which houses vocal cords.
- The trachea bifurcates into two main bronchi at a point called the Carina, leading to smaller bronchioles.
Alveoli and Gas Exchange
- Alveoli are grape-like sacs where gas exchange occurs; they are closely associated with pulmonary capillaries for efficient oxygen transfer.
- Oxygen from ambient air enters alveoli and diffuses into pulmonary capillaries, while carbon dioxide moves from blood to alveoli for exhalation.
Role of Diaphragm in Breathing
- The diaphragm is a dome-shaped muscle crucial for ventilation; its function will be elaborated later in the discussion.
Upper vs. Lower Airway Distinction
- Understanding whether a condition affects upper or lower airways is essential in diagnosing respiratory issues; larynx serves as a boundary between both regions.
Components Supporting Ventilation
- Key components include:
- Chest wall muscles (intercostal muscles)
- Pleura surrounding lungs
- Phrenic nerve connecting brain signals to diaphragm
Definitions: Ventilation, Oxygenation, Respiration
- Ventilation: Refers to getting air in (inhalation) and out (exhalation).
- Oxygenation: Involves increasing oxygen levels in bloodstream via methods like using oxygen tanks or BVM (Bag-Valve-Mask).
Understanding Active Respiration and Breathing Mechanics
The Role of Diffusion in Respiration
- Active respiration involves diffusion, which facilitates the exchange of oxygen into the bloodstream while removing carbon dioxide as a byproduct of metabolism.
Physics of Breathing: Pressure and Volume
- In a smaller space, there are more collisions leading to greater pressure; thus, pressure is inversely proportional to area. As the area decreases, pressure increases.
Exhalation Process
- During exhalation (expiration), the diaphragm relaxes and chest contracts, increasing internal pressure due to reduced volume in the thoracic cavity.
Inhalation Mechanism
- Inhalation occurs when the diaphragm contracts and pulls downwards, expanding the chest cavity. This creates lower pressure inside compared to outside air, allowing air to flow in.
Importance of Diaphragm Movement
- The diaphragm's downward movement increases space within the thoracic cavity, resulting in decreased internal pressure that facilitates inhalation.
Spinal Injuries and Their Impact on Breathing
Key Spinal Levels for Breathing Control
- C3, C4, and C5 spinal nerves are crucial for breathing; injuries at these levels can lead to severe respiratory issues or quadriplegia if higher levels are affected.
Breathing Regulation: CO2 vs. Oxygen Levels
Normal Breathing Stimulus
- Healthy individuals primarily breathe based on CO2 levels monitored by chemoreceptors in arterial blood rather than directly from low oxygen levels.
Hypoxic Drive Explained
- Individuals with certain lung diseases may rely on hypoxic drive—breathing triggered by low oxygen levels instead of high CO2 levels.
Clinical Implications of Hypoxic Drive
Backup System for Breathing Regulation
- When CO2 levels become excessively high over time, the brain switches from monitoring CO2 to relying on oxygen levels as a backup system for initiating breath.
Treatment Considerations for Patients with Hypoxic Drive
Understanding Respiratory Physiology and Metabolism
The Role of Oxygen and CO2 in Patient Treatment
- Discusses the challenge of determining a patient's CO2 levels, emphasizing that it cannot be tested directly in the field.
- Highlights the importance of administering oxygen to patients with breathing difficulties, regardless of outdated medical literature.
Chemoreceptors and Breathing Regulation
- Explains how chemoreceptors monitor O2 and CO2 levels in arterial blood, influencing the stimulus to breathe controlled by the medulla oblongata.
VQ Mismatch: A Complex Medical Concept
- Introduces VQ mismatch, where 'V' stands for ventilation and 'Q' for perfusion; explains its significance in respiratory physiology.
- Describes two scenarios leading to VQ mismatch: good blood supply but poor oxygen intake or vice versa, affecting overall gas exchange efficiency.
Understanding Metabolism: Aerobic vs. Anaerobic
- Mentions the Krebs cycle as a complex topic related to ATP production, which is essential for cellular energy.
- Differentiates between aerobic metabolism (efficient use of oxygen) and anaerobic metabolism (leading to lactic acid buildup due to insufficient oxygen).
Clinical Implications of Lactic Acid Levels
- Connects high lactic acid levels with septic shock patients who are not metabolizing properly due to low oxygen availability.
- Notes that athletes can experience lactic acid buildup during intense training but are not necessarily sick like septic patients.
Monitoring Lactic Acid Levels in Patients
- Discusses how athletes may artificially increase their tolerance to lactic acid through specific training methods.
Understanding Respiratory Patterns and Lung Sounds
Normal Respiratory Rate
- The normal respiratory rate for an adult is between 12 to 20 breaths per minute, emphasizing the importance of measuring breaths at rest rather than BPM.
Breathing Rhythms
- Various breathing rhythms exist, with Kussmaul breathing being a notable example; however, it will be discussed in detail later.
- While there are fewer recognized breathing rhythms compared to cardiac rhythms, understanding these patterns is crucial for assessment.
Quality of Breathing
- Key terms include "labored" (indicating difficulty in breathing) versus "non-labored," which describes normal ease of breath.
- Observing chest expansion is important; deep or shallow breaths can indicate different health conditions.
Difficulty Breathing Calls
- Difficulty in breathing is a common reason for emergency calls; understanding how to assist patients effectively is essential.
Lung Sounds Classification
- Historically, lung sounds were categorized into three types: good lung sounds, bad lung sounds (anything that doesn't sound like good), and absent lung sounds (the most concerning).
- The term "a-" indicates absence in medical terminology; knowing this helps in identifying conditions related to respiration.
Advancements in EMT Training
- EMT training has evolved to include new medications such as albuterol, which requires knowledge of specific lung sounds like wheezing for effective use.
Identifying Lung Sounds
- Understanding various lung sounds—wheezing, diminished sounds, stridor—is critical for diagnosis and treatment decisions.
- Familiarity with normal lung sounds aids in recognizing abnormalities; resources are available online for practice but should be approached critically.
Importance of Stridor and Wheezing
Understanding Airway Problems and COPD
Overview of Airway Issues
- Strider indicates an upper airway problem, while wheezing signifies a lower airway issue. Sleep apnea is characterized by temporary cessation of breathing, often due to tongue obstruction.
- The discussion begins with chronic obstructive pulmonary disease (COPD), which encompasses two major conditions: chronic bronchitis and emphysema.
Chronic Bronchitis Explained
- Chronic bronchitis is defined as a long-term condition that typically develops later in life, often linked to smoking or exposure to pollutants.
- The distinction between acute and chronic conditions is emphasized; acute refers to sudden onset, whereas chronic denotes ongoing issues without a complete cure.
- Unlike viral or bacterial bronchitis seen in children, chronic bronchitis affects older individuals and results from prolonged irritants.
Symptoms and Terminology
- Patients with chronic bronchitis may exhibit cyanosis (blue discoloration), indicating hypoxia. This condition is referred to as "the blue bloater."
- Cyanosis can be central (around lips/face) or peripheral (fingers). Central cyanosis is more critical and visually apparent.
Cilia Functionality
- Cilia are microscopic hairs in the respiratory system that help clear debris from airways. Dysfunction can lead to impaired airflow.
Transitioning to Emphysema
- Chronic bronchitis can progress into emphysema, where patients are termed "pink puffers" due to their appearance when breathing becomes labored.
- Emphysema involves atelectasis—the collapse of alveoli—leading to reduced lung surface area for gas exchange.
Key Differences Between Conditions
- The primary difference between chronic bronchitis and emphysema lies in the structural changes within the lungs; emphysema leads to alveolar destruction while chronic bronchitis primarily causes inflammation.
Hypoxic Drive in COPD Patients
Understanding Respiratory Issues and EMT Response
The Role of Secondary Muscles in Breathing
- Discussion on the use of secondary muscles during breathing, highlighting visible muscle tension when a person struggles to breathe.
- Introduction of cyanosis as a sign of respiratory distress, with mention of "barrel chest" as an interesting phenomenon related to chronic respiratory issues.
- Explanation that consistent weightlifting leads to muscle growth; similarly, individuals with barrel chests develop large chest muscles due to excessive effort in breathing.
- Emphasis on the unhealthy development of these muscles over time due to chronic respiratory strain.
Identifying Dyspnea and Its Implications
- Definition of dyspnea (difficulty in breathing), contrasting it with apnea (inability to breathe); noting that patients may only be able to speak one or two words before needing a breath.
- Importance for EMTs to focus on patient observations rather than distractions; recognizing signs of respiratory issues is crucial for effective care.
Focused Assessment in High-Stress Situations
- Personal anecdote illustrating the necessity for EMTs to maintain focus during emergencies, disregarding surrounding chaos while attending to patient needs.
- Highlighting the importance of observing body positioning as a key indicator of respiratory distress; specific examples provided.
Overlapping Signs and Symptoms
- Reminder that signs and symptoms can overlap across various medical conditions, complicating diagnosis for EMTs who must gather information without making definitive diagnoses.
- Acknowledgment that not all patients present textbook symptoms; real-life cases often deviate from expected presentations.
Treatment Considerations for Respiratory Distress
- Discussion about shallow respirations indicating abnormal breathing patterns; emphasis on immediate action required by EMT personnel when observing such signs.
Professional Demeanor in Patient Care
Importance of Professionalism
- Emphasizes the necessity for healthcare professionals to maintain a professional demeanor regardless of their position, from top surgeons to EMTs.
- Stresses that control over the patient and scene is crucial; if one feels out of control, they should project confidence until a senior takes over.
- Acknowledges the difficulty in maintaining composure and professionalism, highlighting that it requires time and practice.
Patient Comfort
- Highlights the importance of making patients feel comfortable and secure as they rely on healthcare providers for care.
- Discusses oxygen administration based on clinical judgment before assessing lung sounds, indicating proactive patient management.
Understanding COPD
Key Concepts of COPD
- Defines Chronic Obstructive Pulmonary Disease (COPD), mentioning chronic bronchitis and emphysema as its primary components.
- Notes key differences between chronic bronchitis (often blue appearance due to cyanosis) and emphysema (typically pinker complexion).
Asthma: A Serious Condition
Asthma Overview
- Asserts that asthma is a serious condition that can be life-threatening; it should never be treated lightly.
Pathophysiology of Asthma
- Introduces the concept of bronchospasm as central to understanding asthma, explaining how airways constrict during an attack.
- Describes inflammation in asthmatic patients leading to thickened airway walls and mucus accumulation.
Key Terms Related to Asthma
Important Concepts
- Reinforces three critical terms: asthma, lower airway, and wheezing. These concepts are interconnected in understanding respiratory issues related to asthma.
Tools for Assessment
Understanding Respiratory Assessment and Conditions
Monitoring Respiratory Function
- The use of monitoring devices allows for real-time visualization of inhalation, exhalation, and CO2 levels, providing critical insights into respiratory function.
- Normal end-tidal CO2 levels range from 35 to 45 mmHg, with an optimum level at 40 mmHg; understanding these values is essential for assessing patient status.
Recognizing Wheezing Patterns
- Wheezing is typically heard during exhalation and is referred to as an "expiratory wheeze," commonly associated with asthma.
- A single breath consists of one inhalation and one exhalation; recognizing the type of wheezing (e.g., expiratory vs. inspiratory) is crucial in diagnosis.
Signs of Respiratory Distress
- Pursed lip breathing can indicate respiratory distress; patients may close their lips tightly to create back pressure while exhaling.
- Agitation in patients often signals anxiety or worsening respiratory conditions; the tripod position (leaning forward with hands on knees) may be adopted for easier breathing.
Critical Indicators in Asthma Management
- Accessory muscle use, nasal flaring, cyanosis, tachycardia, and tachypnea are key indicators of respiratory distress that healthcare providers should monitor closely.
- "Silent chest" refers to a severe form of asthma where no breath sounds are detected upon auscultation; this condition requires immediate medical intervention.
Understanding Acute Pulmonary Edema
- Acute pulmonary edema (PE), characterized by fluid accumulation in the lungs, can arise suddenly and necessitates rapid assessment and treatment.
Understanding Diuretics and Heart Failure
What is a Diuretic?
- A diuretic is a type of medication that helps remove excess water and fluids from the body by acting on the kidneys.
- Dosage can vary, typically ranging from 20 mg to 80 mg, taken once or twice daily based on fluid retention in patients.
- The most common diuretic mentioned is Lasix (also known as furosemide), which is frequently prescribed for heart-related issues.
Heart Function and Fluid Management
- Issues arise when either side of the heart struggles to pump blood effectively, leading to fluid buildup.
- When the left side of the heart fails, it can cause blood to back up into the lungs, resulting in pulmonary congestion.
- This backup leads to fluid accumulation in the lungs, causing difficulty in breathing and oxygenation problems.
Acute Pulmonary Edema
- Patients with acute pulmonary edema may experience drowning sensations due to fluid filling their lungs.
- Symptoms include difficulty breathing while lying down; patients often need to be propped up for relief.
Treatment Approaches
- New devices like CPAP are now approved for EMT use; they help force air into the lungs and push out excess fluid.
- Proper management of pulmonary edema involves understanding lung sounds such as "rails," which indicate fluid presence.
Clinical Findings
- High blood pressure readings (e.g., systolic pressures around 280 mmHg) are common in patients experiencing acute pulmonary edema.
- A critical clinical sign is "pink frothy sputum," indicating severe respiratory distress due to fluid overload.
The Dangers of Carbon Monoxide
Understanding Carbon Monoxide Toxicity
- Hemoglobin's affinity for carbon monoxide over oxygen poses significant health risks; it prefers CO even at the expense of oxygen transport.
Understanding Carbon Monoxide Poisoning
Introduction to Carbon Monoxide and Its Effects
- The discussion begins with a focus on carbon monoxide (CO) and its impact on the body, emphasizing the need for awareness in environments where CO may be present.
- Laughter indicates a lighter moment before transitioning into serious content about how carbon monoxide affects oxygen transport in the body, leading to cellular death due to lack of oxygen.
Symptoms and Emergency Response
- A critical warning is given: if multiple individuals are found unresponsive in a location, it is likely due to carbon monoxide poisoning; immediate evacuation is essential.
- An anecdote illustrates a real-life scenario involving gas-powered forklifts operating simultaneously in an underground warehouse, highlighting the risks of CO buildup in poorly ventilated spaces.
Case Study: Warehouse Incident
- The speaker recounts responding to an incident where workers experienced dizziness and headaches after exposure to high levels of CO from multiple running forklifts.
- Symptoms such as cherry-red skin are noted as late signs of severe poisoning; early recognition of symptoms can prevent further health complications.
Treatment and Monitoring
- Patients were treated with oxygen therapy; monitoring was crucial for those showing persistent symptoms post-exposure.
- Emphasis on recognizing signs of distress in children during potential CO exposure situations, indicating that they may not show typical responses initially.
Airway Management Techniques
Importance of Airway Management
- Transitioning into airway management techniques, two primary methods are introduced: non-traumatic (head tilt-chin lift) and traumatic (modified jaw thrust).
Equipment Overview
- Discussion includes types of airways used by EMTs: oropharyngeal airway (OPA) and nasopharyngeal airway (NPA), explaining their specific applications based on patient conditions.
Oropharyngeal Airway Functionality
How to Insert Airway Devices
Inserting Oropharyngeal Airway (OPA)
- The OPA can be inserted in two ways: either at 180 degrees along the soft palate and then turned, or at 90 degrees and adjusted as needed.
- It is crucial that the flange of the OPA sits on the lips. Patients without a gag reflex are ideal candidates for this procedure.
- If a patient has a gag reflex, do not attempt re-insertion; instead, remove it completely.
Measuring for Nasopharyngeal Airway (NPA)
- The NPA is placed in the nose and should have its bevel facing towards the sternum. A non-oil-based lubricant is recommended for insertion.
- While everyone can receive an NPA, new protocols advise against its use if head trauma is suspected due to potential complications.
Suctioning Techniques
- Suctioning can be performed using handheld manual suction or mechanical electrical suction. EMTs typically use a French tip catheter for deep suction.
- When suctioning, insert without activating the suction and cover the hole made during insertion; activate suction while withdrawing in a circular motion.
Understanding Oxygen Cylinders
Historical Context of Oxygen Tanks
- Historically, oxygen cylinders were entirely green in the U.S., but now they are often aluminum with only part of them painted green.
- Knowledge of the Pin Index Safety System (PISS) is essential to ensure that only medical-grade oxygen tanks fit into appropriate regulators.
Medical Grade Oxygen
- Medical-grade oxygen is classified as a drug under USP regulations, ensuring safety and efficacy in medical settings.
- The PISS system prevents incorrect connections between different types of gas tanks, safeguarding against misuse.
Pressure Measurement
- Oxygen tank pressure is measured in PSI (pounds per square inch), which remains common despite most medical measurements transitioning to metric units.
Understanding Oxygen Delivery Devices
Overview of Equipment
- The pressure gauge and flow meter are essential for monitoring oxygen delivery, with the flow rate typically set at 15 liters per minute.
- Focus on liters per minute as the primary measure for patient oxygen supply, rather than pounds per square inch (psi).
Non-Rebreather Mask Usage
- The non-rebreather mask is the most commonly used device for patients who are breathing adequately; it delivers approximately 90% oxygen at a flow rate of 15 liters per minute.
- Important components include the reservoir bag, which should be filled to about one-third to two-thirds capacity before use.
Nasal Cannula Considerations
- EMT protocols in New York State restrict nasal cannula usage to specific conditions; primarily when patients cannot tolerate a non-rebreather mask.
- If a patient expresses discomfort with the non-rebreather mask, EMTs should remain calm and explain its benefits while considering switching to a nasal cannula if necessary.
Protocol for Nasal Cannula Application
- The nasal cannula has two prongs that fit into the nostrils and can only be set up to six liters per minute according to state regulations.
- It is crucial not to exceed this limit unless explicitly instructed by medical personnel.
Patient Assessment and Transfer
- When encountering patients on home oxygen therapy (homo), assess their current condition before deciding whether to switch them from their equipment to an ambulance's supply.
Oxygen Delivery and Ventilation Techniques
Understanding Oxygen Equipment Usage
- The speaker discusses the practicality of using a patient's own oxygen equipment instead of transferring theirs, emphasizing the importance of keeping their original setup intact for when they return home.
- It is noted that taking oxygen equipment to the hospital may result in it being lost due to hospital protocols, hence it's advisable to leave it at home.
- The speaker highlights the convenience of shorter oxygen tubing (3-4 feet) compared to longer versions (100 feet), which can be cumbersome for patients moving around their homes.
Key Oxygen Flow Rates and Devices
- A focus on understanding flow rates: 6 liters per minute provides approximately 44% oxygen, while 15 liters can deliver up to 97% oxygen.
- Introduction of Venturi masks used in nursing homes; each color corresponds to a specific percentage of prescribed oxygen, crucial for patient transport.
Tracheostomy Management
- Explanation of tracheostomy procedures where an opening (stoma) is created in the neck for patients who have lost their airway due to various medical conditions.
- Emphasis on proper ventilation techniques through a stoma during cardiac arrest situations, including closing the mouth and nose to prevent air escape.
Nebulizer Use in Emergency Situations
- Discussion about nebulizers and albuterol usage by EMTs; emphasizes correct operation with appropriate flow rates (4-6 liters).
- Caution against using excessive pressure in nebulizers as it can cause malfunction; effective use involves ensuring mist production without exceeding recommended flow rates.
Assessing Breathing Adequacy
- Definition clarification regarding inadequate breathing; normal respiratory rate should be around 12–20 breaths per minute—anything significantly lower indicates potential respiratory failure.
Understanding Ventilation Techniques
The Importance of Proper Ventilation
- Discussion on the term "ventilate" and its significance in medical contexts, emphasizing the need for clarity in terminology.
- Mention of ventilation rates, highlighting that 30 breaths per minute is acceptable, but faster rates may be necessary depending on patient size and condition.
Pathophysiology of Breathing Difficulties
- Explanation of how patients may struggle to get air into their lungs due to diffusion issues, leading to CO2 buildup and potential complications.
- Introduction of a technique where patients can be ventilated every six seconds to ensure proper oxygenation.
Use of Bag-Valve-Mask (BVM)
- Overview of using a BVM with room air upon arrival at a scene; New York State mandates this practice for initial patient assessment.
- Clarification that ambient air contains approximately 21% oxygen, which is sufficient for basic breathing needs.
Enhancing Oxygen Delivery
- When using a reservoir with the BVM, it can deliver close to 100% oxygen continuously due to its design.
Best Practices for Rescuers
- Emphasis on state guidelines preferring pocket facemasks over BVM when only one rescuer is available; highlights challenges in maintaining an effective seal with BVM alone.