EMBRIOLOGÍA: SISTEMA RESPIRATORIO
Formation of the Respiratory System
Introduction to Embryology and the Respiratory System
- Buen día a todos, en este video se abordará la embriología del sistema respiratorio. Se comenzará con la formación de las yemas pulmonares y su desarrollo durante el ciclo médico.
Development Timeline and Key Factors
- La formación del sistema respiratorio inicia en la cuarta semana de gestación, donde el mesodermo incrementa el ácido retinoico, lo que induce al endodermo del tubo intestinal a expresar el factor de transcripción TVX4.
Formation of the Respiratory Diverticulum
- El aumento del ácido retinoico provoca que la parte anterior del intestino genere una invaginación conocida como divertículo respiratorio o yema pulmonar, esencial para el desarrollo de estructuras como la laringe y los pulmones.
Communication with the Anterior Intestine
- Inicialmente, la yema pulmonar tiene comunicación con el intestino anterior; sin embargo, a medida que se expande caudalmente, se forman crestas que generan un tabique transesofágico dividiendo esta estructura en esófago (dorsal) y tráquea (ventral).
Clinical Correlation: Esophageal Atresia
- Se menciona una correlación clínica importante: la atresia esofágica, caracterizada por una separación anómala entre esófago y tráquea debido al tabique transesofágico. Esto puede llevar a complicaciones significativas como fístulas traqueoesofágicas.
Types of Esophageal Atresia Presentations
Common Presentations of Esophageal Atresia
- La presentación más común implica que el segmento proximal termina en un saco ciego mientras que el distal forma una fístula con la tráquea. Esta condición requiere atención médica inmediata para evitar complicaciones severas.
Rare Forms of Esophageal Atresia
- Otras presentaciones incluyen:
- Aislamiento completo de ambos segmentos sin comunicación.
- Fístula única entre esófago y tráquea sin separación.
- Segmento proximal formando fístula mientras que distal termina en saco ciego.
- Ambas porciones tienen fístulas independientes con la tráquea.
Development of Laryngeal Structures
Internal Lining and Cartilage Formation
Development of the Respiratory System
Mesenchyme Proliferation and Epithelium Formation
- The mesenchyme proliferates rapidly, leading to a temporary occlusion of the lumen by the epithelium. This internal lining is crucial for subsequent development.
Formation of Ventricles and Vocal Cords
- The rapid proliferation results in structures known as "ventricles" which are later limited by insular folds that develop into false and true vocal cords.
Trachea and Bronchial Development
- The trachea forms from the fusion of tracheoesophageal ridges, creating a septum that leads to the formation of primary bronchial buds on each side.
Primary and Secondary Bronchi
- By the fifth week, these primary bronchial buds differentiate into right and left primary bronchi; the right bronchus develops three secondary bronchi while the left develops two.
Growth Patterns of Lungs
- As lung development progresses, they expand caudally and laterally within the body cavity, facilitated by pericardial channels.
Separation of Pleurae
- The pleura separates from peritoneal structures due to pleuropericardial folds, forming visceral (covering lungs) and parietal (lining thoracic wall) pleurae.
Branching of Bronchioles
- Secondary bronchi continue to branch into tertiary or segmental bronchi—10 on the right side and 8 on the left—culminating in 17 generations by six months gestation.
Maturation Process Post-Birth
- After birth, further branching occurs with significant growth positioning; at birth, tracheal bifurcation aligns with vertebra four.
Pulmonary Development Stages
Continued Division of Bronchioles
- By seven months gestation, terminal bronchioles divide into respiratory bronchioles; vascularization increases as capillaries surround these structures.
Alveolar Formation
- Terminal bronchioles give rise to alveolar ducts leading to primitive alveoli. Each alveolus is closely associated with flat alveolar cells for efficient gas exchange.
Gas Exchange Readiness
Understanding Fetal Lung Development
The Role of Surfactant in Lung Maturation
- Carbon dioxide levels and the development of mature capillaries allow for gas exchange, enabling survival for babies born as early as seven months.
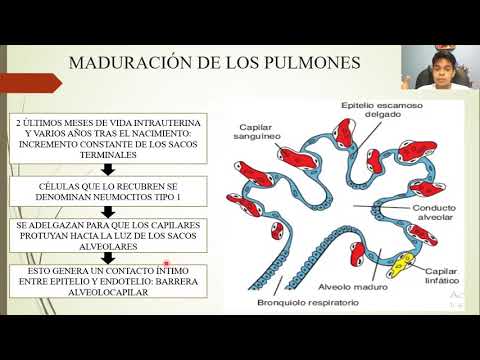
- In the last two months of intrauterine life, type 1 alveolar cells begin to thin out, facilitating better capillary penetration and gas exchange.
- By the end of the sixth month, type 2 alveolar cells synthesize surfactant, which is crucial for reducing surface tension in the alveoli.
Importance of Amniotic Fluid and Macrophages
- Before birth, lungs are filled with fluid containing chloride, proteins, and mucus from bronchial secretions; this fluid volume increases significantly in the final weeks.
- Surfactant enters amniotic fluid where it interacts with macrophages that migrate to synthesize immune proteins like interleukin 1 beta, promoting uterine contractions through increased prostaglandins.
Fetal Breathing Movements
- Fetal breathing movements start before birth to stimulate lung development and condition respiratory muscles despite being surrounded by amniotic fluid instead of air.
- Most aspirated amniotic fluid is absorbed by blood and lymphatic capillaries; a small amount crosses into trachea during aspiration.
Mechanism of Surfactant Action Post-Birth
- After birth, surfactant forms a thin layer over cell membranes in the alveoli to facilitate liquid absorption and prevent high surface tension upon first breaths.
- This mechanism prevents alveolar collapse during initial breaths by maintaining low surface tension due to surfactant action.
Clinical Significance
- The role of type 2 alveolar cells and surfactant is critical in preventing respiratory distress syndrome (previously known as hyaline membrane disease), particularly common in premature infants.