¿Qué es el vértigo paroxístico benigno?
Understanding Benign Paroxysmal Positional Vertigo
Introduction to Dizziness and BPPV
- Dr. Marco introduces the topic of dizziness, specifically focusing on benign paroxysmal positional vertigo (BPPV), a common inner ear disease.
- The video aims to explore the diagnosis, prevention, and treatment of BPPV.
Characteristics and Symptoms of BPPV
- BPPV is identified as a leading cause of vertigo, accounting for approximately 20% of cases seen in medical settings.
- It can occur alongside other ear diseases like Meniere's disease, necessitating careful evaluation for additional pathologies.
- Characteristic symptoms include significant dizziness triggered by specific head movements, particularly when transitioning between lying down and sitting or standing.
- Patients may experience nystagmus—an involuntary eye movement that occurs during episodes of vertigo lasting only a few seconds before subsiding.
- Symptoms are often paroxysmal; they come and go but can also lead to mild constant dizziness when not experiencing full episodes.
Duration and Recurrence
- Episodes typically resolve within one to two weeks without treatment but may recur after several months.
- Proper identification and treatment are crucial since most patients can be effectively cured with appropriate maneuvers.
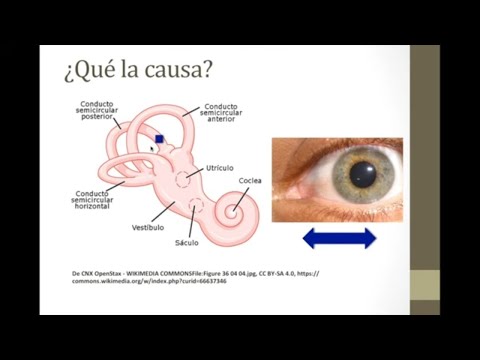
Anatomy of the Inner Ear
- The inner ear consists of three parts: outer ear, middle ear, and inner ear; the vestibular organ is responsible for balance.
- Key structures include semicircular canals (stationary, horizontal, oblique), utricle, and saccule containing otoliths that help detect head position relative to gravity.
Mechanism Behind BPPV
- Movement activates nerves in these structures which communicate with the brain via the vestibular nerve about head position and necessary eye movements.
- When stationary, utricle and saccule indicate no movement; however, head turns activate semicircular canals filled with fluid that signal changes in position.
Causes of Vertigo in BPPV
Understanding Benign Paroxysmal Positional Vertigo (BPPV)
Mechanism of Dizziness and Nystagmus
- The sensation of dizziness occurs when head movements create a mismatch in the brain's perception of motion, leading to confusion about direction. This can result in nystagmus, where the eyes move uncontrollably left and right.
- A small stone in the posterior semicircular canal causes this dizziness; it disrupts normal signaling from the vestibular system, making the patient feel as if their surroundings are spinning.
- Symptoms intensify with head movement due to the stone's interaction with nerves in the semicircular canal, while remaining still may alleviate symptoms temporarily.
- When attempting to stand or move again, symptoms return as the stone impacts more nerve endings, causing intense dizziness and nystagmus once more. This condition is known as benign paroxysmal positional vertigo (BPPV).
Risk Factors for BPPV
- BPPV is more prevalent in women and typically appears after age 50; it is rare before age 35 but can occur due to head trauma in younger individuals.
- Associated ear pathologies such as Meniere's disease or otitis media can also lead to BPPV by displacing stones into semicircular canals. Frequent occurrences warrant further investigation into underlying conditions if standard maneuvers do not yield results.
- Cardiovascular risk factors like dyslipidemia and hypertension may increase episodes of paroxysmal vertigo over time, especially if these conditions are poorly managed.
- Migraine history can be linked to later development of BPPV; patients with long-term migraines may experience vertigo that suggests a connection between these two conditions.
Signs, Symptoms, and Diagnosis
- Patients typically report dizziness triggered by specific head movements; this dizziness varies from mild to severe but is characteristically paroxysmal—intensifying during movement then subsiding afterward.
- Nystagmus observed during episodes often presents as rotatory movements of the eyes; nausea and vomiting frequently accompany intense dizziness but are not mandatory for diagnosis.
Diagnosis and Treatment of Paroxysmal Vertigo
Diagnosis Process
- The diagnosis can often be performed at the patient's home with assistance from a trained family member, particularly using the Epley maneuver, which is typically curative for most patients.
- Patients are usually older adults (over 50 years), but cases of paroxysmal vertigo have been reported in children.
- During the examination, the patient’s head is turned to a 45-degree angle towards their right shoulder to assess involvement of the right ear.
- The patient lies down with their head hanging about 20 degrees below horizontal; if they experience dizziness or nystagmus, it indicates right ear involvement.
- If the first maneuver is negative, the process is repeated by turning the patient's head to the left shoulder to check for left ear involvement.
Understanding Nystagmus and Further Testing
- It is possible for both ears to be involved, but typically only one ear shows signs of benign paroxysmal vertigo.
- For patients with persistent dizziness regardless of maneuvers, further investigation may include CT scans or nystagmography to identify other pathologies.
- Nystagmography can be video-based or electrical; however, most patients do not require this as the Dix-Hallpike maneuver suffices for diagnosis.
Treatment Options
- Most patients respond well to a single canalith repositioning maneuver (Epley maneuver); some may need additional sessions if symptoms persist.
- Patients can perform these maneuvers frequently at home under guidance from trained family members, potentially leading to improved outcomes over time.
- After successful treatment and symptom relief, patients should avoid rapid head movements and keep their heads elevated for at least 48 hours to prevent recurrence of symptoms.
Ongoing Management and Considerations
Understanding the Epley Maneuver and Its Applications
Overview of Vertigo Treatment Options
- The Epley maneuver is effective for treating certain types of vertigo, but other causes may require different approaches.
- Antihistamines can serve as vestibular suppressants; however, they are generally ineffective for benign paroxysmal vertigo and often just mask symptoms.
- A thorough medical history and examination are crucial to determine if vestibular suppressants will be beneficial for patients with combined conditions like Meniere's disease.
Performing the Epley Maneuver
- The Epley maneuver begins similarly to the Dix-Hallpike test, with the patient seated and their head turned towards the affected ear.
- After laying the patient down with their head hanging slightly downwards, a 180-degree turn of the head is performed to face the opposite side.
- The patient's body is then turned towards the right side while maintaining head positioning to facilitate fluid movement in the inner ear.
Steps in Detail
- After holding this position for about a minute, further adjustments are made by turning the patient's chin towards their shoulder before lifting them up.
- If initial attempts do not yield complete improvement, repeating these steps usually results in significant relief for most patients after one or two maneuvers.
Follow-Up Actions
- If patients do not achieve full recovery post-maneuver, they can practice at home under supervision from family members while ensuring no other dizziness causes exist.
Conclusion and Acknowledgments
- Future videos will provide more detailed demonstrations of these maneuvers. Gratitude is expressed to supporters who contribute monthly donations to help create educational content.
Introduction to Clinica Cares and Women's Health
Overview of Clinica Cares
- The speaker announces the launch of their online clinic, Clinica Cares, which is now active and available for consultations.
- The website for scheduling consultations is provided as clinicacares.com.mx, emphasizing accessibility for potential patients.
Services Offered
- Clinica Cares primarily focuses on women's health issues but also offers general consultation services.
- Viewers are encouraged to reach out with any questions or doubts regarding the services offered at the clinic.
Closing Remarks