Part 4 Carbapenems, Cephalosporins, Fluoroquinolones
Curbing Opponents: Understanding Carbapenems and Cephalosporins
Overview of Carbapenems
- Carbapenems are a new class of broad-spectrum antibiotics effective against both gram-positive and gram-negative bacteria, with meropenem being a notable example.
- The first drug discussed has limited use due to severe risks for potentially fatal gastrointestinal (GI) toxicity; it is bactericidal and treats serious infections.
- Indications for this antibiotic include serious infections in intra-abdominal, urinary tract, skin, joint, and gynecological areas.
- Contraindications include known allergies, seizure disorders, and caution during pregnancy; regular urine function tests are necessary.
- Pseudomembranous colitis is a significant concern associated with antibiotic therapy leading to severe diarrhea and dehydration.
Adverse Effects and Drug Interactions
- Antibiotics can disrupt normal intestinal flora leading to Clostridium difficile infections causing nausea and vomiting.
- CNS effects such as dizziness, headaches, altered mental states, and seizures have been reported when combined with other drugs.
- Probenecid should not be combined with meropenem due to the risk of toxic levels; alternative antibiotics may be needed if patients are on anticonvulsants like valproic acid.
Introduction to Cephalosporins
- Following carbapenems, cephalosporins were introduced; they share structural similarities with penicillin but differ in effectiveness across generations.
- First-generation cephalosporins are largely effective against gram-positive bacteria while second-generation shows reduced efficacy against them but remains potent against gram-negative bacteria.
Generational Differences in Cephalosporins
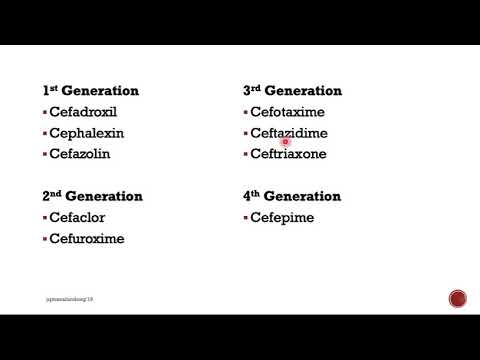
- Third-generation cephalosporins are effective against previously mentioned strains but weaker against gram-positive bacteria. Fourth generation is still developing with cephepene as an active drug.
- Notable examples include cefalexin (first), cefuroxime (second), ceftazidime (third), and cefepime (fourth).
Therapeutic Actions & Pharmacokinetics
- All cephalosporins exhibit bactericidal actions; their selection depends on the sensitivity of the involved organism determined through culture tests.
- Pharmacokinetics involve liver metabolism with excretion via urine; they cross the placenta and breast milk. Absorption varies by generation.
Indications and Cautions for Antibiotic Use
Key Considerations in Antibiotic Administration
- Known allergies to cephalosporins and penicillins should be assessed due to their similarities.
- Adverse effects on the gastrointestinal (GI) tract are common, including nausea, vomiting, diarrhea, and abdominal pain.
- Monitor for nephrotoxicity and superinfections; intravenous administration may lead to injection site reactions.
- Patients on oral anticoagulants face an increased risk of bleeding; monitor for signs like easy bruising.
- Educate patients to avoid alcohol for 72 hours post-antibiotic treatment to prevent disulfiram-like reactions.
Fluoroquinolones: Overview and Usage
Characteristics of Fluoroquinolone Antibiotics
- Ciprofloxacin is a widely used fluoroquinolone with broad-spectrum activity against gram-negative bacteria.
- Effective in treating urinary tract infections, respiratory infections, and even anthrax prevention.
- Pharmacokinetics include absorption from the GI tract, metabolism in the liver, and excretion via urine; crosses the placenta.
- Levofloxacin is preferred for severe infections when oral intake isn't possible; finafloxacin is used as otic drops for ear infections.
Safety Concerns with Fluoroquinolones
- Not recommended for patients under 18 years due to potential cartilage development issues.
- Common adverse effects include CNS symptoms like headache and dizziness, along with GI disturbances such as nausea and diarrhea.
Risks Associated with Fluoroquinolone Use
Potential Complications
- Increased risk of tendinitis and tendon rupture in patients over 60 or those on corticosteroids; instruct patients to report any pain or weakness.
- Drug interactions can decrease therapeutic effects when taken with iron salts or antacids; separate doses by at least four hours.