Otitis externa / Otitis media / Mastoiditis / Otoesclerosis
Introduction to Otology and Clinical Cases
Overview of Topics
- The session begins with an introduction to otology, focusing on surgical specialties in otorhinolaryngology. Key topics include external otitis, acute otitis media, complications of otitis media such as gastritis and abscesses, and other related conditions.
- Emphasis is placed on clinical practice guidelines relevant to these conditions, particularly acute otitis media in children, which often appears in clinical case scenarios. Understanding treatment options like amoxicillin is highlighted as crucial.
Acute External Otitis
- Acute external otitis is defined as a diffuse inflammation of the external auditory canal that may involve the auricle or tympanic membrane due to infection following a breach in the mechanical barrier. This definition is essential for understanding the condition's etiology.
- Bacterial infections account for 98% of cases; Pseudomonas aeruginosa (20-60%) and Staphylococcus aureus (10-70%) are identified as primary etiological agents. While Staphylococcus is more common in adults, Pseudomonas is emphasized in clinical guidelines.
Clinical Presentation and Diagnosis
- The typical presentation includes sudden onset symptoms within 48 hours after swimming or trauma from cotton swabs, characterized by severe ear pain (otalgia) that may radiate to the jaw or face. Pruritus can also be present. The "tragus sign"—pain upon pressure—is a key diagnostic indicator for external otitis.
- Diagnosis relies primarily on clinical evaluation; physical examination reveals inflamed and painful auditory canals that may appear closed due to swelling. If an autoscopic exam shows normal findings, further investigation into temporomandibular joint dysfunction or dental issues may be warranted.
Treatment Approaches
Non-pharmacological Management
- Non-drug treatments include applying acetic acid drops (or vinegar) into the affected ear every eight hours and using cotton with petroleum jelly during bathing to keep the ear dry while allowing ventilation post-bath. Minimizing manipulation of the ear canal is advised alongside avoiding swimming activities until recovery occurs.
Pharmacological Options
- First-line pharmacological treatment involves antibiotic-steroid combinations such as neomycin-polymyxin B-hydrocortisone drops administered every eight hours for seven days; alternatives include ciprofloxacin with hydrocortisone if necessary.
- Caution is advised against using certain drops if there’s a perforated tympanic membrane due to potential toxicity from neomycin; thus careful assessment before prescribing these medications is critical for patient safety.
Pain Management and Otitis Externa: Clinical Insights
Pain Management Strategies
- The combination of paracetamol and naproxeno is recommended for pain management over 48 to 72 hours, with dextropropoxifeno as an alternative for severe cases.
- It is crucial to monitor patients for alarm signs such as increased pain or lack of improvement within two hours, indicating a need for reassessment.
- Patients with otitis externa should show significant improvement within two to three days; otherwise, treatment may need adjustment.
- Alarm symptoms include worsening hearing loss, fever, or swelling; these require referral to family medicine or otorhinolaryngology if no improvement occurs.
Diagnosis and Treatment of Otitis Externa
- Initial assessment includes checking for symptoms like otalgia and pruritus, often linked to swimming or trauma from objects like cotton swabs.
- If cellulitis of the auricle is present, referral to a higher level of care is necessary to rule out malignant otitis externa caused by Pseudomonas aeruginosa.
- A case study highlights the importance of recognizing malignant otitis externa in immunocompromised patients who may not respond well to standard treatments.
Understanding Malignant Otitis Externa
- The majority of malignant otitis externa cases are due to Pseudomonas; thus, antibiotics must have anti-Pseudomonal action (e.g., ciprofloxacin).
- Mismanagement can occur if inappropriate antibiotics are prescribed that do not target the causative organism effectively.
Treatment Protocol Overview
- For non-complicated cases of otitis externa without perforation, topical treatments like neomycin-polymyxin can be effective alongside general measures (e.g., keeping the ear dry).
- In cases where there’s obstruction due to foreign bodies or perforation in the tympanic membrane, referral is warranted.
Complications and Special Considerations
- Persistent symptoms after initial treatment necessitate further evaluation; failure to improve within two hours indicates potential complications requiring second-level care.
- Malignant otitis externa primarily affects diabetic males with immunosuppression; understanding this demographic helps in early identification and intervention strategies.
Otitis Media and Its Clinical Implications
Overview of Otitis Types
- The speaker emphasizes the importance of understanding otitis externa maligna and localized otitis, noting that while questions often focus on otitis media, awareness of these types is beneficial.
Understanding Otitis Media
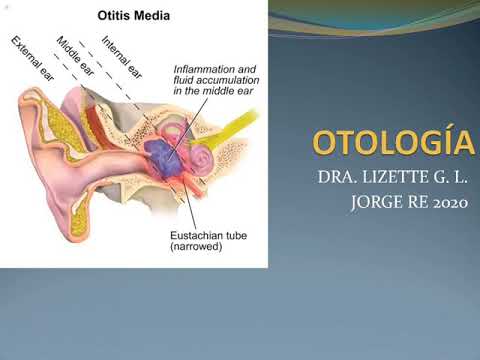
- Otitis media is highlighted as a significant topic, characterized by acute infection in the middle ear with effusion—presence of fluid without symptoms indicating an active infection.
Etiology and Statistics
- The etiology breakdown shows 59% bacterial and 41% viral causes; this statistic underscores the commonality of bacterial infections in practice despite variability.
- Key bacterial pathogens include Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis. Viral causes primarily involve respiratory syncytial virus (RSV).
Age-related Epidemiology
- Children aged 6 months to 3 years are most affected by acute otitis media, with up to 85% of cases occurring in this demographic due to immature Eustachian tube function.
Clinical Presentation
- Differentiating between otitis media and external otitis is crucial; typically, patients with otitis media are young children or infants, while external cases are more common in adults or adolescents.
Symptoms and Diagnosis
- Common symptoms include ear pain (otalgia), fever, and hearing loss. Diagnosis relies heavily on clinical evaluation through pneumatic otoscopy.
Phases of Otitis Media
- Two phases are identified:
- Early phase marked by intense pulsatile ear pain.
- Late phase characterized by perforation and purulent discharge leading to symptom improvement.
Treatment Guidelines
- Treatment decisions should be based on clinical history combined with physical examination findings. Pneumatic otoscopy remains the diagnostic method of choice.
Antibiotic Protocol
- Amoxicillin is recommended for children under six months old. For those older than six months but less than two years, antibiotics are prescribed only if fever exceeds 39°C or if there’s no improvement after initial treatment within 48 hours.
Severe Cases Management
- In severe cases (fever over 39°C or lack of improvement after treatment), amoxicillin-clavulanate may be added after failure to respond to initial therapy within a specified timeframe.
Otitis Media and Its Complications
Treatment Approaches for Severe Cases
- Amoxicillin with clavulanic acid is recommended for severe patients; macrolides are used for those allergic to penicillin.
- Streptococcus pneumoniae is identified as the primary cause of otitis media, with influenza virus also noted as a significant etiological factor.
Clinical Signs and Diagnosis
- Key clinical signs include fever and auricular retraction, particularly in children under two years old.
- CT scans (with or without contrast) are essential for diagnosing structural damage when there’s no improvement after 72 hours.
Surgical Interventions
- If no improvement occurs within 48 hours, surgical options such as fine needle aspiration or mastoidectomy may be necessary.
- Complications like abscess formation can arise from infections caused by Streptococcus pneumoniae.
Additional Complications of Mastoiditis
- The first complication includes periorbital abscesses characterized by fever, anterior auricular retraction, and otalgia.
- The second major complication involves the development of a neck abscess due to Streptococcus spp., presenting with torticollis and cervical swelling.
Understanding Autoimmunity in Otosclerosis
Overview of Otosclerosis
- Otosclerosis is described as a metabolic bone disease affecting the otic capsule and ossicles, leading to hearing loss.
Genetic Factors
- It has low prevalence (0.13%) but shows a familial link with autosomal dominant inheritance patterns that exhibit incomplete penetrance.
Clinical Presentation
- Characteristically presents with hearing loss typically occurring in the third decade of life, more common in women at a ratio of 2:1.
Risk Factors and Pathology
- Infection risk factors include measles virus exposure; histopathological classification impacts treatment approaches significantly.
This structured summary provides an organized overview of key points discussed in the transcript regarding otitis media complications and insights into otosclerosis. Each bullet point links directly to its corresponding timestamp for easy reference.
Understanding Otoesclerosis and Its Clinical Implications
Pathophysiology of Otoesclerosis
- The process of otoesclerosis involves the hardening of bone, particularly affecting the stapes (stirrup bone) and its connection to the oval window, leading to reduced mobility.
- When there are foci of otoesclerosis in both the bony labyrinth and the oval window, they act like glue, causing fixation that results in limited movement within this structure.
Clinical Presentation
- Patients typically experience slowly progressive hearing loss (hipoacusia), often becoming noticeable in their third decade of life. About 70% will have bilateral symptoms.
- Hearing loss may present with a drop of up to 25 decibels; tinnitus occurs in approximately 80% of cases, along with balance disorders affecting 10-25% due to labyrinthine involvement.
Diagnostic Approach
- Diagnosis is primarily through audiometry, which reveals characteristic patterns associated with otoesclerosis. Key findings include a conductive hearing loss pattern at around 2000 Hz.
- Audiometric tests show a significant drop in bone conduction thresholds at specific frequencies, indicating conductive hearing loss typical for otoesclerosis.
Audiometric Testing Techniques
- The Rinne test evaluates air versus bone conduction; normally, air conduction should be better than bone conduction. In otoesclerosis, this may not hold true due to fixation.
- The Weber test lateralizes sound towards the affected ear when there is conductive hearing loss because sound transmission through bone is enhanced compared to air.
Treatment Options
- Medical management includes sodium chloride and auditory aids; however, surgical intervention is often necessary for effective treatment.
- Stapedectomy is highlighted as a preferred surgical option due to fewer complications compared to other procedures. Understanding surgical criteria is essential for appropriate patient selection.
Case Studies Overview
- A review of clinical cases will follow; these cases illustrate various presentations and management strategies for patients with otoesclerosis.
Otitis Externa and Related Conditions
Overview of Symptoms and Diagnosis
- Discussion on symptoms including fever, inflammation of the ear, and fluid drainage indicating possible otitis externa or media. The presence of mastoid pain is noted in diabetic patients.
- Consideration of malignant otitis externa as a potential diagnosis, especially in diabetic patients with cranial nerve paralysis. Emphasis on the need for thorough physical examination.
- Identification of pseudomonas aeruginosa as a likely causative agent in cases of malignant otitis externa, particularly in patients with specific risk factors.
Clinical Case Analysis
- Presentation of a 35-year-old patient with progressive bilateral hearing loss exacerbated by pregnancy. Examination reveals abnormal findings in the left ear.
- Findings suggest conductive hearing loss in the left ear; tympanometry shows decreased compliance and absence of reflexes, indicative of otosclerosis.
Key Takeaways from Otolaryngology
- Importance of understanding less common conditions like otosclerosis alongside more frequently encountered issues such as otitis media.
- Acknowledgment that while general practitioners encounter various ENT conditions, specialists have deeper insights into complex pathologies and procedures.
Conclusion
- The discussion emphasizes the significance of recognizing symptoms early to prevent complications associated with ear infections and related disorders.