Semana 10 Nutrición 03/10/22
Understanding Diabetes and Its Impact
In this section, the instructor delves into the importance of understanding diabetes, focusing on the endocrine system and the role of the pancreas in maintaining homeostasis through insulin and glucagon.
The Pancreatic Endocrine System
- The pancreas consists of islets of Langerhans responsible for producing various hormones. Key cells include Alfa cells producing glucagon, Beta cells producing insulin (majority in the pancreas), Delta cells secreting somatostatin, G cells for gastrin, and F cells for peptide secretion.
- Homeostasis in the pancreas involves insulin secretion when blood glucose is high to convert glucose to glycogen for storage. Conversely, glucagon is secreted when blood glucose is low to break down glycogen into glucose for release into the bloodstream.
Functions of Insulin
- Insulin acts as an anabolic hormone stimulating glucose uptake into cells, glycolysis for energy production, lipid synthesis, amino acid uptake, and protein synthesis. It inhibits processes like gluconeogenesis (using sources other than glucose for energy), glycogenolysis (breaking down stored glycogen), lipolysis (degrading fatty acids), and proteolysis.
- Insulin's anabolic nature leads to weight loss in diabetic patients when insulin production decreases or stops. This hormone promotes synthesis activities while inhibiting alternative energy sources utilization.
Types and Causes of Diabetes
Here, the discussion shifts towards defining diabetes as a syndrome caused by chronic hyperglycemia due to insulin deficiency or resistance. The instructor elaborates on Type 1 diabetes resulting from autoimmune destruction of beta cells versus Type 2 diabetes linked to insulin resistance.
Types and Causes
- Diabetes manifests as a syndrome with chronic hyperglycemia due to either insufficient insulin secretion or impaired function/action. Type 1 diabetes stems from autoimmune destruction of beta cells necessitating external insulin supply. In contrast, Type 2 diabetes primarily results from insulin resistance rather than absolute deficiency.
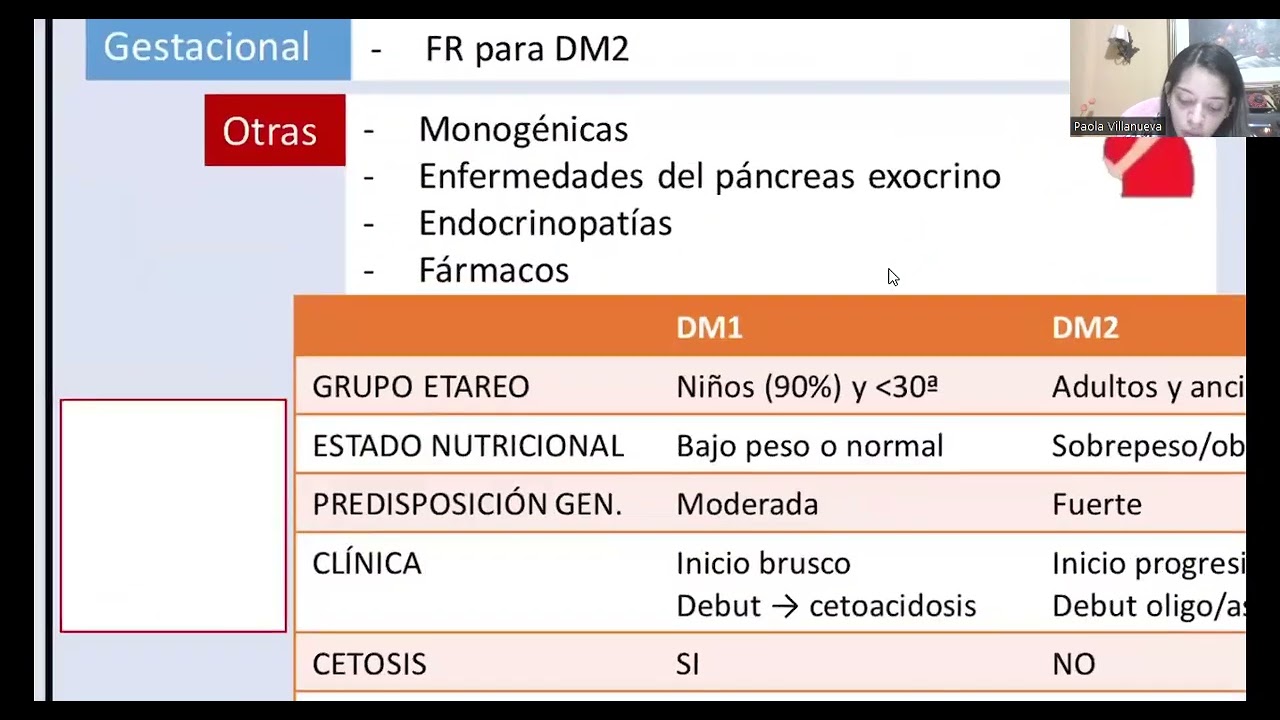
- Other less common types include gestational diabetes during late pregnancy without prior history and genetic or pancreatic disorders causing atypical forms. Understanding these distinctions aids in diagnosing and managing different types effectively.
Autonomy and Development of Diabetes
In this section, the speaker discusses the progression from having antibodies against islets to the development of diabetes, focusing on the time frame and key indicators leading to intolerance to glucose.
Progression Towards Diabetes
- Patients with prediabetes or type 2 diabetes show clinical symptoms such as increased concentrations of diabetics.
- Prediabetes begins when a patient loses around 50% of beta cells, progressing to diabetes when only 10% of endocrine pancreas function remains.
- Patients with insulin resistance require higher insulin levels due to excessive glucose in their bodies, leading to increased insulin production.
Clinical Symptoms and Differentiation
- Classic symptoms of diabetes include polyuria, polydipsia, polyphagia, and weight loss (the 4 Ps).
- Type 1 diabetes is more common in young patients while type 2 typically affects adults with poor lifestyle habits.
Clinical Characteristics and Diagnosis of Diabetes
This part delves into the clinical characteristics that differentiate between type 1 and type 2 diabetes based on age groups, nutritional status, genetic predisposition, and onset symptoms.
Distinctive Features of Diabetes Types
- Type 1 diabetes commonly occurs in younger individuals with normal appearance or even underweight. In contrast, type 2 often affects overweight or obese adults due to poor dietary habits.
Genetic Predisposition and Onset Symptoms
- The onset of type 1 diabetes is abrupt and may involve diabetic ketoacidosis. Conversely, type 2 symptoms can be asymptomatic until hyperglycemia occurs.
Treatment Approaches for Different Diabetes Types
This segment explores treatment strategies for type 1 and type 2 diabetes focusing on insulin therapy for type 1 and initial dietary management for type 2.
Treatment Strategies
- Type 1 diabetes necessitates insulin therapy due to an absolute deficit in insulin production. In contrast, type 2 can initially be managed through diet before progressing to medications like antibiotics.
Impact on Insulin Secretion
- Decreased insulin secretion in diabetes affects incretin hormones' action prolonging insulin's presence in blood circulation. However, this effect diminishes in diabetic conditions.
Physiological Effects of Reduced Insulin Action
This part elucidates how reduced insulin action leads to various physiological changes affecting lipid metabolism, glucose absorption rates, muscle function neurotransmission alterations.
Physiological Consequences
Diagnosis and Complications of Diabetes
In this section, the speaker discusses the diagnostic criteria for diabetes, including fasting glucose levels, oral glucose tolerance test results, and glycosylated hemoglobin levels. Additionally, they touch upon the complications associated with diabetes, categorizing them into microvascular and macrovascular complications.
Diagnostic Criteria for Diabetes
- Fasting glucose levels:
- Normal: <100 mg/dL
- Prediabetes: 100-125 mg/dL
- Diabetes: ≥126 mg/dL
- Oral Glucose Tolerance Test:
- Normal: <140 mg/dL at two hours
- Prediabetes: 140-199 mg/dL
- Diabetes: ≥200 mg/dL
- Glycosylated Hemoglobin (HbA1c):
- Normal: <5.7%
- Prediabetes: 5.7-6.4%
- Diabetes: ≥6.5%
Diagnosis of Diabetes
- Diagnostic process:
- Initial test: Fasting glucose level
- Confirmation may require additional tests like oral glucose tolerance test or repeated fasting glucose tests.
- Confirming prediabetes:
- If initial test shows prediabetes range, an oral glucose tolerance test can confirm.
Complications of Diabetes
- Types of complications:
- Microvascular (retinopathy, nephropathy, neuropathy)
- Macrovascular (coronary artery disease, cerebrovascular disease)
Pathophysiology and Diagnosis of Diabetic Ketoacidosis
This segment delves into the pathophysiology and clinical presentation of diabetic ketoacidosis (DKA), emphasizing its association with insulin deficiency leading to gluconeogenesis and lipolysis. The discussion also covers diagnostic criteria for DKA based on laboratory findings.
Pathophysiology of Diabetic Ketoacidosis
- Insulin deficiency in DKA:
- Results in increased gluconeogenesis and lipolysis.
- Accumulation of ketone bodies due to fat breakdown leads to acidosis.
Clinical Presentation of DKA
- Symptoms include:
- Abdominal pain, nausea, vomiting.
- Kussmaul breathing and fruity breath odor from acetone.
Laboratory Diagnosis of DKA
- Diagnostic criteria:
- Elevated blood glucose (>250 mg/dL).
Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State
In this section, the speaker discusses the differences between diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS), focusing on their diagnostic criteria and treatment approaches.
Diabetic Ketoacidosis (DKA)
- DKA is characterized by ketones in urine and blood, with glucose levels typically above 10.
- Patients with DKA may experience marked dehydration due to osmotic diuresis caused by high blood glucose levels.
- Diagnostic criteria for DKA include glucose levels over 600 and plasma osmolarity above 320.
Treatment Approaches
- Type 1 diabetes is treated with basal insulin along with prandial insulin for meals or continuous subcutaneous infusion.
- Metformin is the first-line therapy for type 2 diabetes, followed by combination therapies if needed.
Diabetes Management Strategies
This part delves into the management strategies for diabetes, including medication escalation based on patient response.
Medication Escalation
- If initial therapy fails in type 2 diabetes, a triple therapy approach may be considered before transitioning to basal insulin.
- Patients with elevated hemoglobin A1c (>8.5%) may require dual therapy or insulinotherapy directly based on severity indicators like high glucose levels or symptoms of HHS.
Fructose and Glycemic Index
The discussion shifts towards fructose's impact on health, particularly its effects on triglycerides and insulin resistance, as well as an explanation of glycemic index.
Fructose Impact
- Excessive fructose consumption can elevate triglyceride levels, induce uric acid production, and lead to insulin resistance.
Glycemic Index Explanation
- The glycemic index indicates how much a food item raises blood glucose levels; foods are classified as high (>70), medium (56-69), or low (<56).
Understanding Glycemic Index Values
Clarification regarding glycemic index values and their implications for blood sugar control.
Glycemic Index Values
- An example of a high glycemic index food is bread; fruits without skin have higher indexes than those consumed whole.
Limiting Fructose Consumption
In this segment, the speaker emphasizes the importance of limiting fructose consumption due to its potential negative effects on triglyceride levels.
The Impact of Excessive Fructose Consumption
- Excessive fructose intake can lead to elevated triglyceride levels.