NEUMONÍA ADQUIRIDA EN LA COMUNIDAD (FISIOPATOLOGÍA PARTE 1)| GuiaMed
Introduction to Pneumonia Pathophysiology
Overview of the Presentation
- The speaker, Christian Poos, introduces the topic of pneumonia and its pathophysiology, expressing enthusiasm for teaching this important medical subject.
- The presentation will cover definitions, pathophysiology, histopathology, morphological types of pneumonia, causes (including community-acquired and nosocomial), clinical manifestations, and severity assessment criteria.
Definition and Causes of Pneumonia
- Pneumonia is defined as a lung infection that leads to inflammation of lung tissue. It can be caused by viral or bacterial infections.
- Other potential causes include radiotherapy or allergies; however, infections are the primary concern leading to significant damage in pulmonary parenchyma.
Understanding the Defense Mechanisms Against Infections
Anatomical Overview
- A brief anatomical overview is provided: nasal passages lead to the pharynx and larynx, followed by the trachea branching into bronchi and ultimately alveoli.
Infection Entry Points
- Viral infections are often a precursor to bacterial infections; inhalation of contaminants can introduce pathogens into the lungs.
- Aspiration from the oropharynx is highlighted as a common route for infection, particularly dangerous for older adults.
Body's Defense Mechanisms Against Pathogens
Initial Defense Strategies
- The body's first line of defense includes nasal structures like turbinates (cornetes) and vibrissae (nose hairs), which trap larger particles.
Secondary Defenses
- If smaller pathogens bypass initial defenses, the tracheobronchial epithelium acts as a secondary barrier through cilia that help expel mucus containing trapped microorganisms.
Advanced Defense Mechanisms in Alveoli
Cellular Composition of Alveoli
- Alveoli consist of type I pneumocytes lining their walls and type II pneumocytes producing surfactant. Macrophages within alveoli play a crucial role in immune response.
Activation Upon Infection
Understanding Macrophage Function in Alveoli
Role of Macrophages
- The most crucial cells within the alveoli are macrophages, responsible for phagocytosing microorganisms that enter the lungs.
- While effective at eliminating pathogens, macrophages have a limited capacity to handle large numbers of microorganisms.
Response to Overwhelming Pathogens
- When bacteria exceed the phagocytic capacity of macrophages, they adapt their response to maintain homeostasis.
- Macrophages release various inflammatory mediators such as interleukin 1 and tumor necrosis factor (TNF), which initiate an inflammatory response.
Inflammatory Mediators and Their Effects
- Interleukin 1 and TNF work to prevent bacterial escape from alveoli by promoting inflammation.
- These mediators recruit leukocytes to the alveoli, enhancing the immune response against bacteria but also causing capillary leakage.
Consequences of Leukocyte Recruitment
- The recruitment process leads to capillary leakage, resulting in fluid accumulation in the alveoli.
- This fluid buildup can obstruct gas exchange and is a clinical hallmark of pneumonia.
Clinical Manifestations of Pneumonia
Symptoms and Physical Findings
- Fluid accumulation in alveoli causes characteristic clinical signs such as crackling sounds during auscultation and hypoxemia.
Histopathology of Pneumonia
Stages of Pneumonia Development
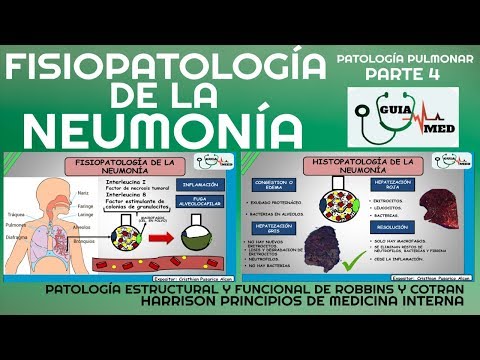
- The histopathological progression includes four key stages: congestion/edema, red hepatization, gray hepatization, and resolution.
Initial Stage: Congestion/Edema
- Pneumonia begins with congestion or edema characterized by protein-rich exudate leaking from capillaries into alveoli filled with bacteria.
Red Hepatization Phase
- Following congestion, red hepatization occurs where erythrocytes leak into the alveoli alongside proteins and leukocytes.
- This phase is difficult to observe early on due to rapid progression from edema to red hepatization.
Gray Hepatization Phase
- In this stage, no new erythrocytes are produced; existing ones degrade while remaining trapped in inflamed tissue.
Understanding the Phases of Pneumonia
The Role of Neutrophils and Bacteria Elimination
- Neutrophils remain abundant in the alveoli during this phase, while bacteria are nearly eradicated, marking a significant step towards tissue repair.
- Although there is effective removal of the aggressive agent, some bacteria may still persist; this is indicated by a grayish appearance in the lungs due to fibrin deposits and erythrocyte lysis.
Resolution Phase of Pneumonia
- In the resolution phase, macrophages take over as leukocytes disappear, effectively cleaning up remaining neutrophils, bacteria, and fibrin from the alveoli.
- This marks a complete elimination of bacteria from the alveoli, preparing them for normal function again after inflammation caused by interleukin 1 and tumor necrosis factor.
Morphological Forms of Pneumonia
- Pneumonia can manifest in two primary forms: lobar pneumonia and bronchopneumonia. Each has distinct characteristics affecting lung consolidation.
Bronchopneumonia Characteristics
- Bronchopneumonia presents as multiple patches or areas affected across different lobes rather than being localized to one specific area.
Lobar Pneumonia Characteristics
- In contrast, lobar pneumonia shows solidification concentrated in one specific portion or an entire lobe of the lung.
Consequences of Incomplete Resolution
- Failure to progress through all phases (red hepatization, gray hepatization, resolution) can lead to tissue destruction and necrosis.
- This incomplete resolution may result in further infection spread beyond pulmonary parenchyma into pleural cavities or even systemic bacteremia.
Upcoming Discussions on Clinical Manifestations
- Future content will cover clinical manifestations associated with pneumonia types such as hospital-acquired pneumonia (HAP), community-acquired pneumonia (CAP), and nosocomial infections.
- The discussion will also include criteria for evaluating pneumonia severity along with other relevant points.
Engagement Encouragement