Trichuris trichiura: Morfología, Ciclo de vida, Patogenia, Clínica, Diagnóstico, Tratamiento
Introduction to Trichuris trichiura
Overview of the Parasite
- The class discusses the intestinal parasitosis caused by the nematode Trichuris trichiura, commonly known as whipworm.
- Nematodes are elongated parasites that primarily infect the mucosa of the large intestine, particularly in the cecum and colon.
Infection Characteristics
- The infection can be asymptomatic or present with enteric symptoms; this will be elaborated upon in clinical discussions.
- Trichuris trichiura is cosmopolitan, found globally but predominantly in warm, humid regions where open defecation occurs.
Demographics and Transmission
- The infection is more common among children aged 5 to 14 years, with humans being the primary reservoir for the parasite.
- Transmission occurs orally; eggs must remain in soil for 10 to 14 days before becoming infectious.
Factors Influencing Infection
Determinants of Infection
- Key factors include fecal contamination of soil, humidity levels necessary for egg viability, and temperature conditions.
- Consumption of contaminated food and water also plays a significant role in transmission.
Conditioning Factors
- Lack of sanitation systems contributes significantly to infection rates.
- Poor personal hygiene practices and inadequate washing of food further increase risk. Socioeconomic status also influences exposure levels.
Morphology of Trichuris trichiura
Physical Characteristics
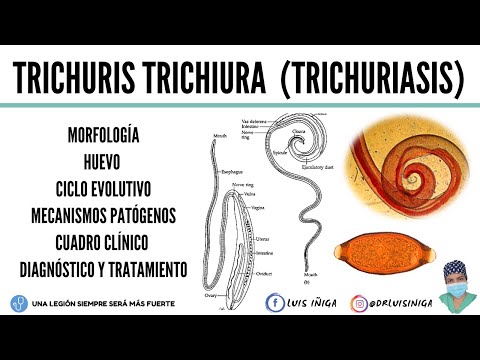
- There are distinct male and female forms; females are generally larger (3 to 5 cm), while males range from 1.5 to 5 cm.
- The anterior end of T. trichiura is slender, resembling a hair—hence its name "whipworm."
Reproductive Anatomy
- Female anatomy includes a mouth without lips leading into an esophagus connected to intestines and reproductive organs like ovaries and uterus.
Understanding the Life Cycle and Pathogenic Mechanisms of Trichuris trichiura
Morphology and Egg Structure
- The anterior end of the Trichuris trichiura parasite is referred to as a "lancet," which it uses to attach to the mucosa of the large intestine.
- The eggs of Trichuris trichiura are brown, elliptical in shape, resembling an American football, measuring approximately 45-60 microns in length and 20-30 microns in width.
- The egg has two ends known as "caps," which help break open to release the larva inside. The shell consists of three layers: outer, middle, and inner (containing the germ cell).
- The outer and middle layers provide protection against unfavorable environmental conditions for egg survival.
Life Cycle Overview
- Adult parasites reside in the colon's mucosa, primarily in the cecum but can also invade the rectum if infection is severe. Both male and female adults copulate here.
- Non-embryonated eggs are expelled through feces into moist soil where they require temperatures between 10°C to 30°C for development over 14 to 15 days or longer.
- Eggs transform from non-embryonated to larvated forms, becoming infective when contaminating soil, water, or food sources that humans may ingest.
Infection Process
- Upon ingestion by humans, larvated eggs travel through the stomach where gastric acids degrade their caps allowing larvae to emerge.
- This degradation process is aided by stomach bacteria; once released, larvae develop into first-stage (L1), then progress through second (L2), third (L3), and fourth stages (L4).
Pathogenic Mechanisms
Mechanical Mechanisms
- Mechanical pathogenic mechanisms include:
- Penetration of intestinal mucosa causing trauma leading to hyperemia (increased blood flow).
- Microtraumas caused by lancet-like structures damaging small blood vessels; some literature suggests T. trichiura may be hematophagous (blood-feeding).
- Distension and weakening of rectal musculature potentially resulting in rectal prolapse.
Chemical Mechanism
- A singular chemical mechanism involves host response forming granulomas around parasites without eliminating them.
Clinical Manifestations
- Clinical presentations can be asymptomatic or symptomatic; symptomatic cases often result in colitis due to inflammation at colon level.
Colitis and Its Symptoms
Overview of Colitis Symptoms
- Colitis primarily presents with mucosal hyperemia and eosinophilia, leading to localized colicky abdominal pain, often in the right iliac fossa, but can also be diffuse.
- Symptoms may include enteric colic with bloody diarrhea, tenesmus (ineffective straining), and potential rectal prolapse. Anemia can occur due to vascular trauma and parasitic blood loss.
Pathophysiology of Symptoms
- The trauma to blood vessels results in microcytic anemia, contributing to malnutrition and anorexia. This combination increases intestinal peristalsis, causing diarrhea and spasms that lead to abdominal pain.
- Altered intestinal function can result in ineffective defecation urges (tenesmus), leading to painful, unproductive straining (pujo). Rectal prolapse may expose the mucosa to infections and worsen bleeding.
Additional Symptoms
- Non-specific symptoms such as anorexia, asthenia (weakness), pallor, weight loss, and acropachy (clubbing of fingers) are associated with malnutrition from micro-traumas.
Diagnosis of Trichuriasis
Diagnostic Parameters
- Diagnosis involves three parameters: clinical signs/symptoms observed during examination; epidemiological data focusing on individuals from tropical regions; laboratory tests for confirmation.
Laboratory Methods
- Direct stool examination reveals eggs or parasites attached to the rectal mucosa in cases of rectal prolapse.
- The Kato-Katz method measures infection intensity by counting eggs per gram of feces; over 10,000 eggs/gram indicates moderate to severe infection.
Treatment Options for Trichuriasis
Medications Used
- Mebendazole is commonly used at a dosage of 100 mg twice daily for three days; children may receive a single dose of 500 mg.
- Albendazole is another option at 400 mg once daily for three days. It inhibits tubulin protein polymerization in parasites.
Alternative Treatments
- Other medications include fluvenazole at 300 mg once daily for three days and pyrantel pamoate which alters parasite metabolism at doses between 200–400 mg divided into two doses over three days.
Management Strategies for Rectal Prolapse
Treatment Approach
- Manual reduction is recommended for rectal prolapse along with securing the area using adhesive strips to prevent recurrence.
Preventive Measures Against Trichuriasis
- Control excreta disposal practices to reduce soil contamination.
- Enhance public health education regarding hygiene practices.
- Ensure access to potable water sources.